|
Back to Fall Congress
Outcomes following Hypospadias Repair: A 10 year national review of specialist pediatric centers in England
Shanthi Beglinger, BSc1, David J. Wilkinson, MB ChB, BMedSci(Hons), MRCS (Eng)2, Rachel Hudson, BSc3, David H. Edgar, MA, DPhil3, Simon E. Kenny, MB ChB, BSc, MD, FRCS (Paed Surg), FAAP2.
1University of Liverpool Medical School, Liverpool, United Kingdom, 2Alder Hey Children's Hospital, Liverpool, United Kingdom, 3University of Liverpool, Liverpool, United Kingdom.
Introduction: A review of surgical outcomes following hypospadias surgery in the published literature reveals a wide range in the reported complication rates. This may be explained by the wide variation in: surgical technique, definition of severity and length of follow up, making comparison between centers or individual surgeons difficult. With such variability in practice and the growing emphasis on monitoring and reporting outcomes it is important to have a benchmark against which to compare both current and future practice.
Materials and Methods: The study population included all children under the age of 19 years undergoing a primary repair for hypospadias between 1999 and 2009 in the 22 specialist centers for pediatric urology in England. Clinical and administrative data were extracted from the English Hospital Episode Statistic Database (HES), which is a national data repository, collated by the UK Department of Health, recording the diagnostic codes (ICD10) and procedure codes (OPCS4.6) associated with each hospital admission within. HES data for each admission are linked via a unique patient identifier allowing all subsequent admissions to any English NHS facility to be tracked, even if the patient changes center. Children with an additional diagnosis within the disorders of sexual differentiation spectrum; bladder exstrophy; or epispadias, were excluded from the study. Primary outcome measures were the surgical correction of: urethral fistula; urethral stricture; meatal stenosis; or more than two hypospadias repairs. Statistical analysis was performed using GraphPad Prism Version 5 (GraphPad Inc, USA). Correlation was determined using linear regression analysis with P<0.05 taken as significant. Data are reported as median (interquartile range, IQR) unless otherwise stated.
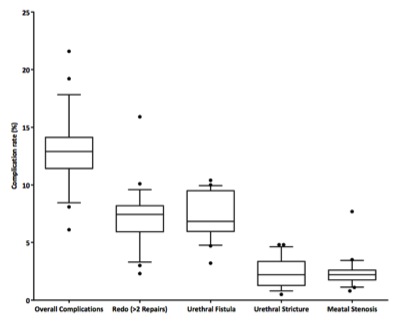
Results: The 22 Specialist pediatric urology centers in England performed a median of 54 (36-85) primary repairs/year during the study period. In total 15,213 primary hypospadias repairs were performed at a median age of 20 (17.3-25.0) months. The median proportion of patients requiring surgical intervention for a complication was 12.9% (Fig.1.) Urethral fistula was the most common complication (6.9%, Fig.1). A significant reduction in complication rate was found to be associated with rising caseload (1% fall in complications per 20 additional cases/annum, p = 0.01, r2 =0.28). Further analysis of subtypes: balanic, penile, penoscrotal and perineal was also performed.
Conclusion: Despite the hetrogenity in surgical techniques employed
This study provides outcome data (median and IQR) at a population level thereby allowing the establishment of a ‘benchmark’ for primary hypospadias surgery. The size of the study helps mitigate the effect of heterogeneity of technique and helps to set a standard against which current and future outcomes can be compared. In keeping with other studies, we identified a significant reduction in complications to be associated with high volume centers.
Figure 1. Comparison of complication rates following primary hypospadias surgery. Centres below the 2.5th or above the 97.5th centiles are plotted individually. Boxes represent the interquartile range and median is expressed as the horizontal line.
Back to Fall Congress
|

