
Robotic-assisted redo pyeloplasty with buccal mucosa graft
Jennifer Ahn, MD, Thomas Lendvay, MD.
Seattle Children's Hospital, Seattle, WA, USA.
Introduction: While the success rate of pyeloplasty is high, treatment of failed pyeloplasty is less effective, as finding healthy, well-vascularized tissue for reconstruction can be challenging. Buccal mucosa grafts (BMG) have been used for >20 years with success in urethral and vaginal reconstruction and have been recently used for ureteral reconstruction in the adult population. We sought to evaluate our experience with BMG in robotic-assisted redo pyeloplasty.
Methods: A retrospective review of all patients undergoing robotic-assisted redo pyeloplasty with BMG at our institution was performed. Patient demographics, details of initial UPJO presentation, and presentation of UPJO recurrence were recorded. Intra-operative details of robotic-assisted redo pyeloplasty were recorded, as were most recent follow-up and imaging.
Operative details: For all patients, the following ports were used: one 8.5mm camera, two 8mm robotic, and one 5mm assistant. Initial dissection was performed laparoscopically and robotically, and the UPJ was incised longitudinally along the anterior surface. The robot was undocked, and BMG was harvested from the inner cheek. The robot was then re-docked, and grafts were delivered via the 8mm robotic ports and anastomosed as anterior onlay grafts using 5-0 or 6-0 absorbable monofilament suture. Omentum was quilted over the graft as a vascular backing. Double pigtail stents were placed intra-operatively and left in situ for 8 weeks. Foley catheters were removed on post-operative day 3. All patients received intravenous ampicillin and gentamicin pre-operatively, with antibiotics discontinued within 24 hours.
Results: A total of three patients underwent robotic-assisted re-do pyeloplasty with BMG. Patient characteristics are seen in Table 1. Mean number of prior surgeries for UPJO repair was 2 (1-3), and mean length of stricture was 4.3cm (2.5-6). No patient had any peri-operative complications. At a median follow-up of 9 months (4-25), all patients are asymptomatic with stable or improved ultrasound.
Conclusions: Robotic-assisted redo pyeloplasty with buccal mucosa graft is safe and feasible in the pediatric population. Long-term follow-up is needed to determine the durability of these grafts. 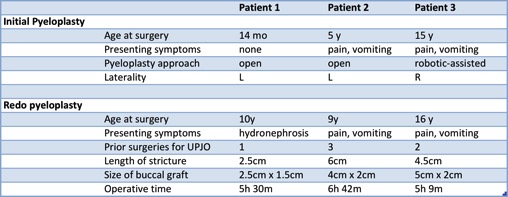
Back to 2016 Fall Congress