
Neonatal Screening - Ambiguity in the Diagnosis of Disorders of Sexual Development
Joseph Ortenberg, MD, Dania Felipe-Ramirez, MD, Aaron D. Martin, MD, MPH, Ricardo Gomez, MD.
Children's Hospital - New Orleans, New Orleans, LA, USA.
Background: In the evaluation of neonates with Disorders of Sexual Development (DSD), pediatric urologists often provide the initial assessment, so practitioners must be aware of the techniques and limitations of testing for DSD. Neonatal screening for Congenital Adrenal Hyperplasia (CAH) has been adopted in all states and minimizes the delay in treatment for a potentially life threatening condition. Techniques for neonatal screening of CAH vary between states, which may create confusion in the diagnosis of DSD. We report our local experience with neonatal screening for CAH and misdiagnoses with false positive and negative results.
Methods: The Genetic Diseases Program of our state Office of Public Health (LaOPH) was queried about suspected and confirmed cases of CAH from inception of this program in 2006 to 2013. Newborn screening was performed by measurement of 17 hydroxyprogesterone levels. The LaOPH data was correlated with the clinical experience of 6 academic pediatric endocrinologists and 3 pediatric urologists in our university system. Hormonal, radiographic and CYP21 testing was performed when indicated.
Results: With an average of 63,531 births per year in our state (Table 1), the average annual rate of suspected positive CAH cases was 1.8 per thousand births. After re-evaluation, the positive predictive value of CAH testing was only 3.2% of the suspected positive cases identified. Unique cases evaluated by pediatric urology, included 3 neonates with genital ambiguity who were falsely negative during newborn screening, representing simple virilizing CAH. One false positive case, initially diagnosed as CAH, was ultimately confirmed to have ovotesticular DSD and underwent definitive surgery. The evaluation and surgical treatment of these unique cases will be presented.
Table 1:
Conclusions: Current newborn screening for CAH varies between states, depending on the type of assay for 17 hydroxyprogesterone and cutoff levels. This may introduce inaccuracy in the diagnosis of CAH, if threshold values are set at a lower level. Pediatric urologists who collaborate in the multispecialty evaluation of DSD should be aware of the techniques of neonatal screening for CAH as well as the concerns about false negative and positive testing. 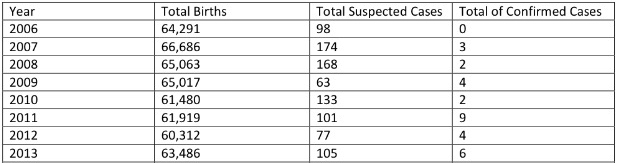
Back to 2016 Fall Congress