
Flow Characteristics of Urethral Catheters of the Same Caliber Vary Between Manufacturers
Carrie A. Stewart, MD1, Elchiro Yamaguchi, PhD2, Jessica Teixeira Vaz, Engineering Student2, Donald P. Gaver, III, PhD2, Joseph Ortenberg, MD3.
1Tulane University School of Medicine, New Orleans, LA, USA, 2Tulane University, New Orleans, LA, USA, 3Louisiana State University School of Medicine, New Orleans, LA, USA.
BACKGROUND:
Clean intermittent catheterization (CIC) is frequently prescribed for bladder dysfunction, either per urethra or via a continent catheterizable channel. Small catheters may be required for infants or reconstructed/continent channels. Success with CIC is highly dependent upon patient and family compliance. Up to 100 minutes per day may be spent performing CIC. The urinary flow rate through the catheter is an important factor, which can decrease CIC time and improve quality of life. There is little objective information in this regard, to guide catheter recommendation or prescription. We propose that catheters of the same labeled diameter do not necessarily exhibit the same flow characteristics, which may ultimately have implications during catheter selection.
METHODS:
Twenty-two commercially available male pediatric urinary catheters from 9 manufacturers were tested (11 straight tip, 11 coude tip). Five of the 22 tested catheters had a hydrophilic coating. All tested catheters shared a 10 French outer diameter. For each, microscopic imaging and a precision caliper were used to measure the inner diameter and tip inlet. A hydraulic system modified from ASTM standard testing specifications was used to simulate bladder catheterization (Figure 1). Measurement of each catheter was repeated 5 times using three different static hydraulic pressures (20, 40 and 50 cmH20). The friction factor derived from the Darcy-Weisbach equation was used to describe real flow resistance imposed by the inlet tip.
RESULTS:
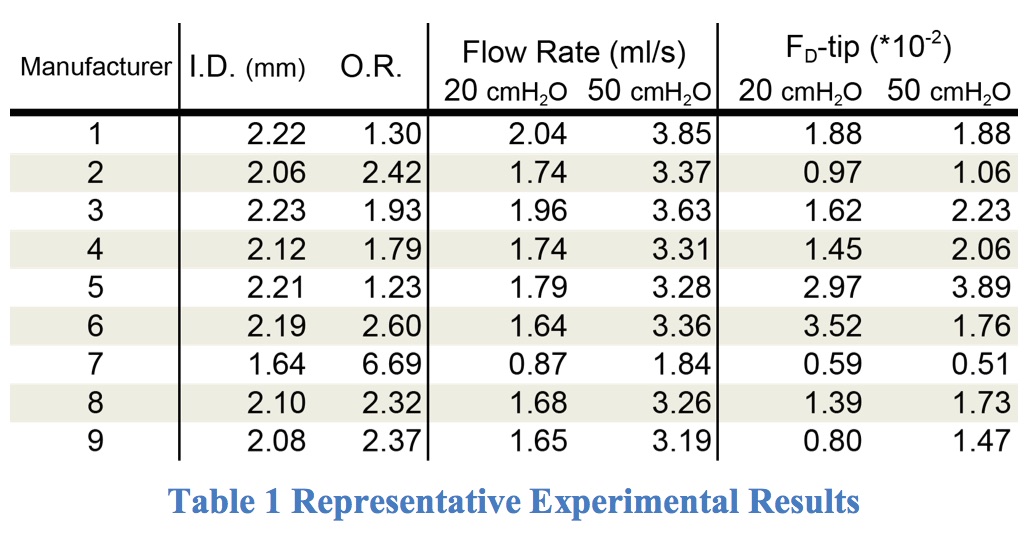
Representative data of the catheter geometry and flow rate measurements are presented in Table 1. There was significant variation between manufacturers in inner diameter (I.D.) and inlet/tube opening ratio (O.R.) in comparison with the same-labeled outer diameter. The maximum difference from the manufacturer average is 22% for I.D., 166% for O.R., and 1.5% for outer diameter. The result of experiments reflected the fluctuations in geometry. For example, the maximum difference of the flow rate is 48% and the friction factor of the inlet tip (FD-tip) is 108%, while the average deviation of each catheter experiment (n=5) was 2.2%. Flows with higher hydraulic pressure (>40 cmH2O) tended to reach a transition regime, 2000<Re<4000, where the linear relationship of pressure and flow rate in laminar flow (Poiseuille equation) no longer applied.
CONCLUSIONS:
The design of some brands of urinary catheters does not optimize urinary flow. The inner diameter and the ratio of inlet/tube opening are two critical parameters, limiting the flow rate. Currently, it is not possible to predict the actual flow rate of urinary catheters based on the packaging information or manufacturer’s specifications. The wide fluctuation of these two parameters between manufacturers should either be regulated or be listed on product packaging along with the outer diameter, to assist physicians and families in selecting the optimal urinary catheter for CIC. 
Back to 2016 Fall Congress