
The Urine Microbiome is Associated with Renal Scarring and Recurrent Febrile Urinary Tract Infection in Children with Vesicoureteral Reflux
Joseph W. McQuaid, MD MPH1, Jonathan M. Mansbach, MD MPH2, Kohei Hasegawa, MD MPH3, Kylie H. Davis, BS1, Nadim J. Ajami, PhD4, Richard S. Lee, MD1.
1Department of Urology, Boston Children's Hospital, Boston, MA, USA, 2Department of Medicine, Boston Children's Hospital, Boston, MA, USA, 3Department of Emergency Medicine, Masschusetts General Hospital, Boston, MA, USA, 4Department of Molecular Virology and Microbiology, Baylor College of Medicine, Houston, TX, USA.
BACKGROUND: Urinary tract infection (UTI) leads to renal scarring in 10-15% of cases. One risk factor for recurrent febrile UTI (fUTI) is vesicoureteral reflux (VUR), but we cannot reliably predict which children with VUR will develop renal scarring or recurrent fUTI. Studies in healthy adults suggest that urine is not sterile, instead consisting of functional bacterial communities (microbiota) associated with risk of or protection against recurrent fUTI. It is unclear, however, in children with VUR if the urine microbiota is associated with renal scarring or recurrent fUTI.
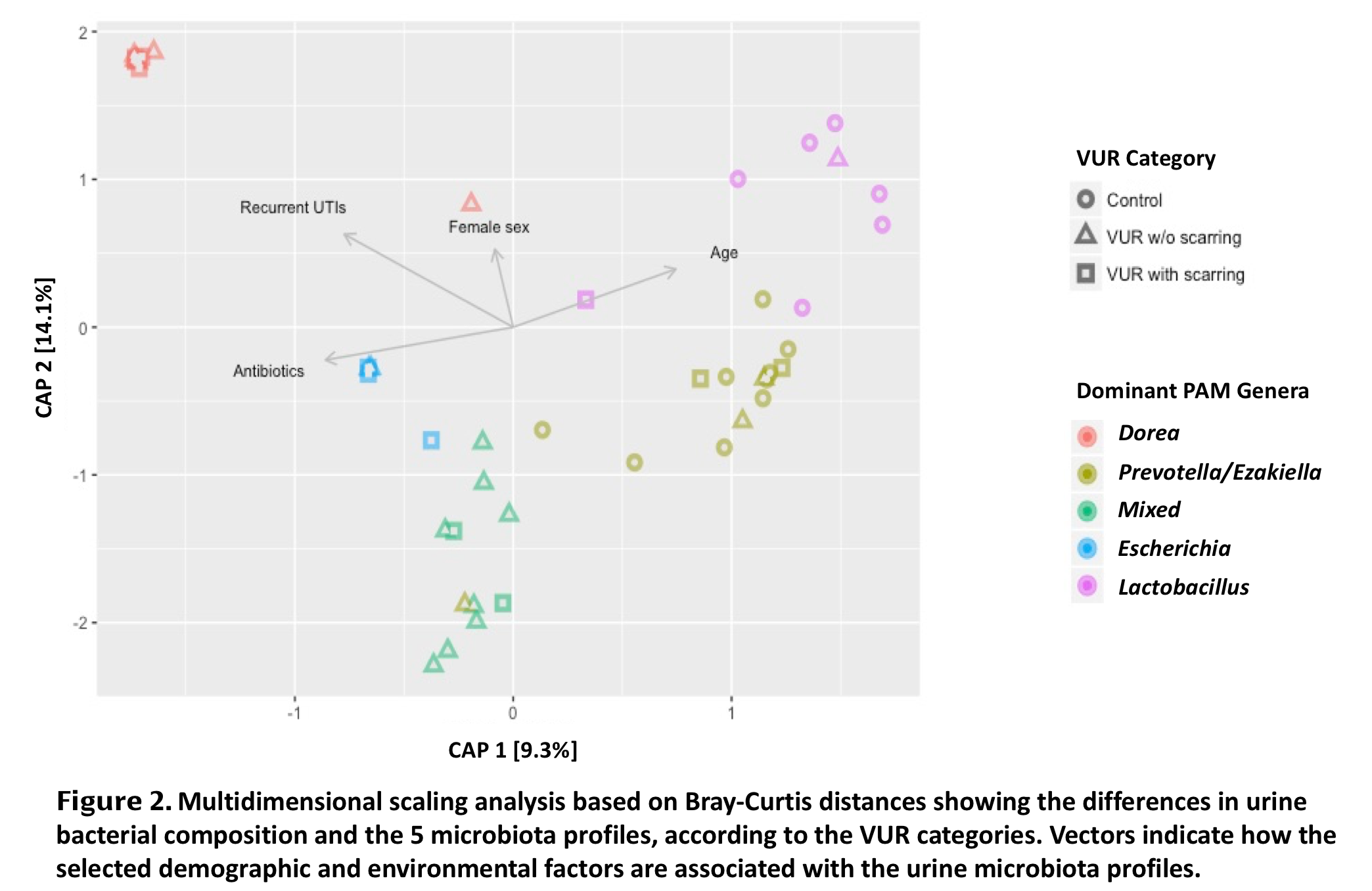
METHODS: We performed 16S rRNA gene sequencing on sterile urine specimens from 33 children during anti-reflux surgery (+/- renal scarring) and 16 pediatric and adult controls (neither VUR nor renal scarring). Subjects were classified into 3 groups according to VUR status on cystography and renal scarring status on dimercaptosuccinic acid (DMSA) study. Recurrent fUTI was defined as more than one documented fUTI at the time of inclusion. We used unbiased clustering by partitioning around medoids (PAM) on Bray-Curtis distances to identify urine microbiota profiles. Between-group variations in microbial community composition were tested using permutational multivariate analysis of variance (perMANOVA).
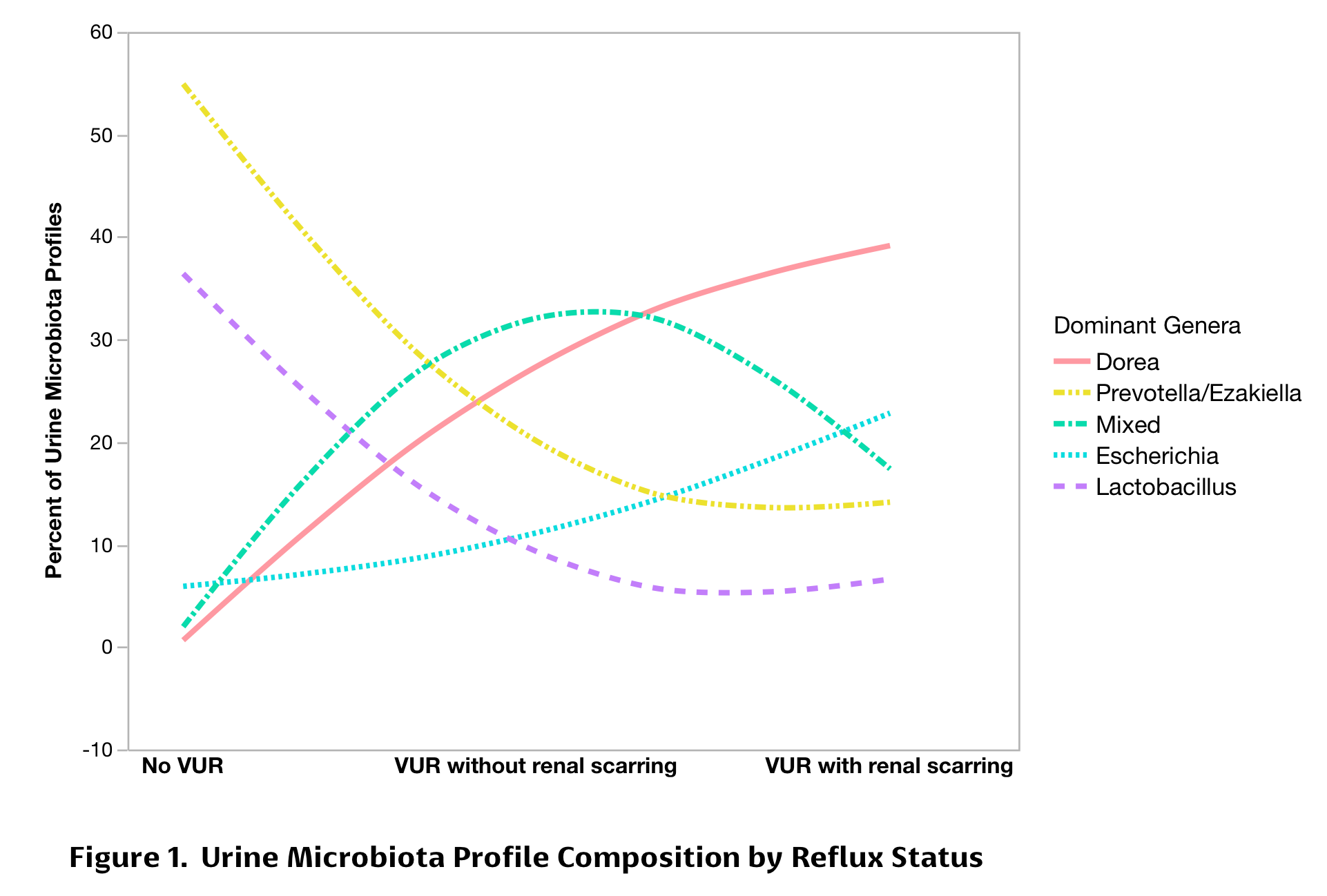
RESULTS: The 49 participants (median age 4.9 years, IQR: 2.9-8.8) included healthy controls (n=16), children with VUR but no scarring (n=20), and children with VUR and scarring (n=13). Compared to controls, patients with VUR were significantly younger, more likely to have recurrent fUTIs, and to be prescribed prophylactic antibiotics (Table 1). We identified five distinct urine microbiota profiles: Dorea-dominant, Escherichia-dominant, Prevotella and Ezakiella-dominant, Lactobacillus-dominant, and mixed profiles (Table 2). Dorea and Escherichia-dominant microbiota occurred more frequently in subjects with VUR +/- scarring. By contrast, Prevotella and Lactobacillus-dominant clusters were more common in healthy controls (p<0.001; Figures 1 and 2). After adjusting for age, sex, antibiotic usage, and history of recurrent fUTIs, the microbial community composition was significantly different among the 3 participant categories (p=0.003). Although VUR status did not perfectly correlate with recurrent fUTI, the microbial community composition was also significantly different between patients with recurrent fUTIs and those without (P=0.001).
CONCLUSIONS: Despite the small sample size, we have demonstrated, for the first time, urine microbiota profiles that significantly differ between healthy controls and children with either VUR +/- renal scarring or recurrent fUTI. Although validation with a larger sample is needed, these results raise the possibility of manipulating the urinary microbiota to affect renal outcomes in children with VUR.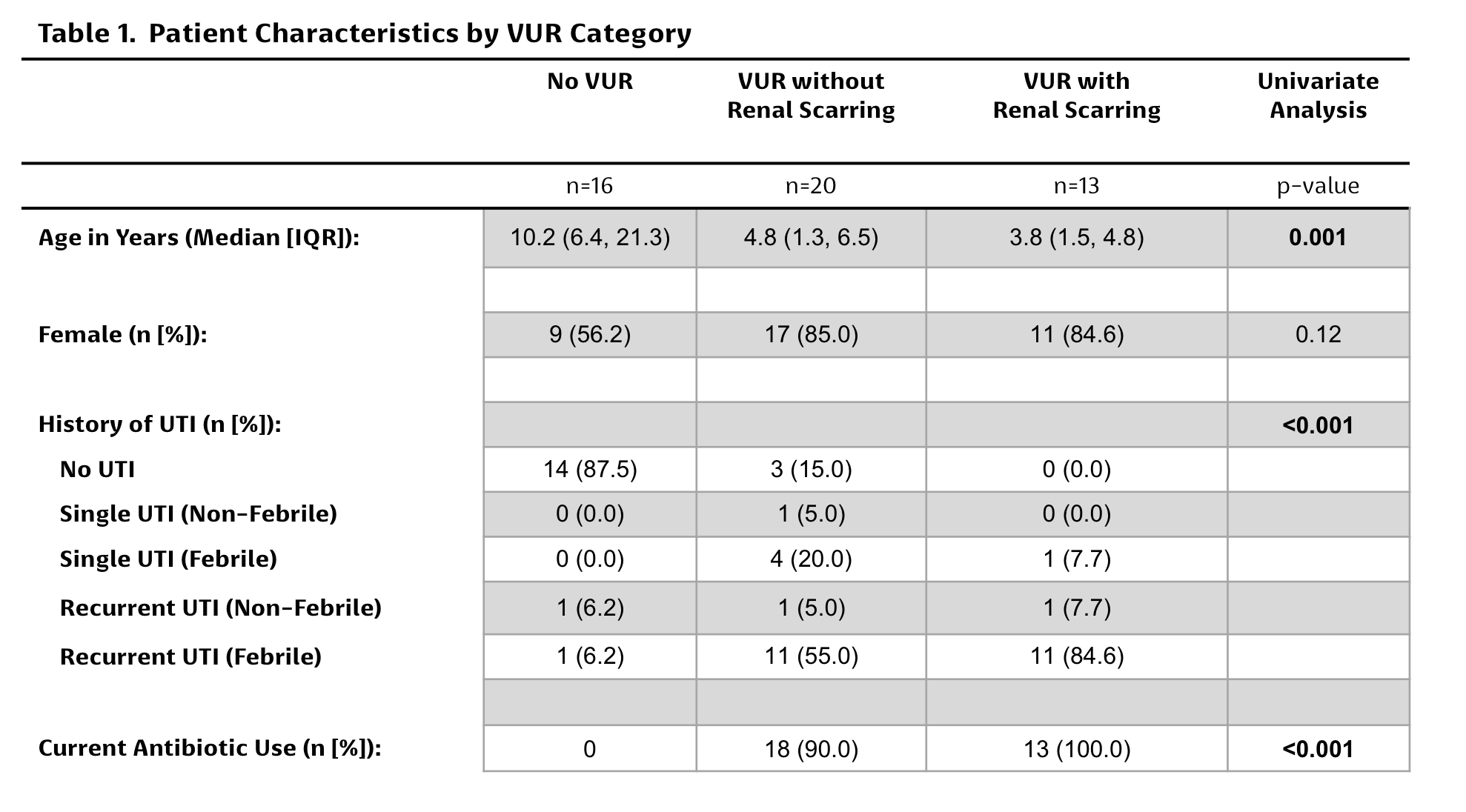

Back to 2017 Program