
Predicting Success in Pediatric Hypospadias Fistula Repair: A Multi-Institutional Review
Ahmad Saeed Imam, BS1, Aaron J. Smith, BS1, Mark A. Rich, MD2, Hubert S. Swana, MD2.
1University of Central Florida College of Medicine, Orlando, FL, USA, 2Arnold Palmer Hospital For Children, Orlando, FL, USA.
Introduction: Urethrocutaneous fistula is the most common complication of hypospadias repair occurring after 6-29% of all hypospadias surgeries. Many different fistula repair techniques have been described. Most series in the literature have described one technique and come from a single institution.
Materials & Methods:
Pediatric hypospadias fistula repairs from five different children's hospitals were retrospectively reviewed over a ten year period (2005-2014). Clinical data and operative reports from initial hypospadias repair and fistula repair surgeries were analyzed. Patient demographics, fistula location and surgical techniques were compared. Special attention was made to the use of adjunct techniques such as Dartos flap coverage and catheter drainage. Complications were recorded. Patients who underwent repair of complete dehiscence or lacked follow-up data were excluded from the study.
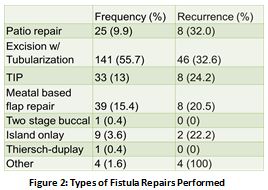
Results: A total of 253 patients were identified. Surgeries were performed by fourteen different board- certified pediatric urologists. The median age was 32.5 months (range 13-202 months). The locations of the fistulae that were repaired, their frequency, and the recurrence rate after repair were analyzed (Figure 1). The different types of repair procedures performed are shown in figure 2.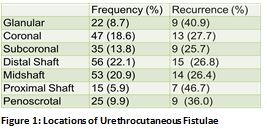
Recurrent fistula occurred in 76 (30%) of all repairs. The risk of recurrence was not found to be statistically significant with any specific location or procedure type. A Dartos flap was used in 180 (71.1%) fistula repair procedures and a catheter was used in 168 (66.4%). The use of a Dartos flap was associated with a significantly lower fistula recurrence rate (p<0.0001) when compared to procedures with no flap coverage (34.4% vs 60.3%). Use of a catheter also had a significantly lower fistula recurrence (p<0.05) compared to no catheter usage (25% vs 40%). The use of both a Dartos flap and a catheter resulted in the lowest fistula recurrence rate (12.3%) (p<0.0001) when compared to using only one or neither (Figure 3). Other complications of the fistula repairs included meatal stenosis, bladder spasm, dysuria, dislodged catheter and urinary tract infection.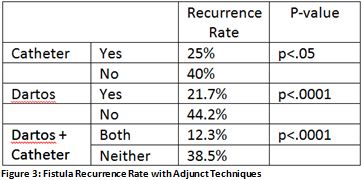
Conclusions: Prior studies have shown a fistula recurrence rate between 11-29% after fistula repair surgery. Our study reveals that the use of a Dartos flap independently decreases the risk of fistula recurrence. Similarly, catheter uses decrease fistula recurrence rates but is associated with slightly higher complication rates. These complications are minor. There lowest fistula recurrence rates are associated with both catheter use and Dartos flap coverage.
Back to 2017 Program