
Does Contralateral Hypertrophy Compensate For Renal Loss In Patients With Solitary Kidneys?
Thomas Gaither, Medical student, Mary K. Wang, MD, Laurence S. Baskin, MD.
University of California, San Francisco, San Francisco, CA, USA.
Background
Renal hypertrophy has been observed in patients with a solitary kidney, such as those with multicystic dysplastic kidney (MCDK) or Wilms tumor. Renal hypertrophy may indicate renal health, although more research is necessary to determine the relationship between kidney length and glomerular filtration rate (GFR). Additionally, once renal hypertrophy occurs does it persist over time?
Materials and methods
We conducted a retrospective cohort study of patients with MCDK and Wilms tumor. MCDK patients were verified by sonographic findings prenatally, and entered our study at first postnatal ultrasound date. Wilms tumor patients entered our study at time of nephrectomy, and pathology was confirmed. Only MCDK patients with greater than 7 years of follow-up were included. This was to match follow-up in our Wilms cohort. Contralateral hypertrophy was defined as either 1 or 2 standard deviations (SD) above normal mean kidney lengths. We compared the natural history of hypertrophy between the two cohorts. Any patient in our medical records with a renal length measurement and creatinine were included for a sub-analysis. We used linear regression to evaluate the relationship between creatinine clearance and renal length after controlling for age.
Results
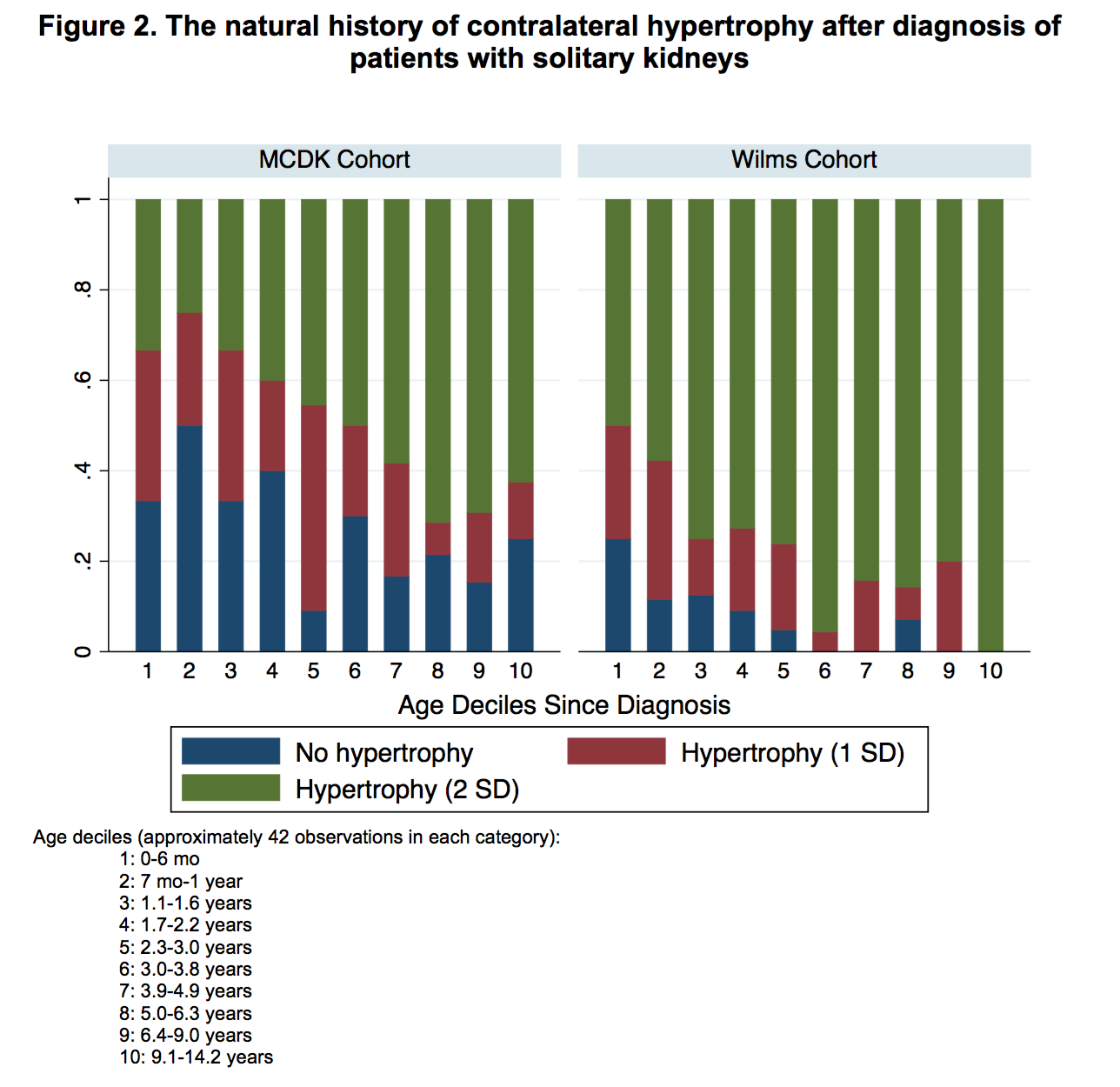
Forty-eight patients (56%) were diagnosed with Wilms tumor at a median age of diagnosis 2.7 years (interquartile range 1.7-5.6). Thirty-seven patients (44%) with MCDK patients met study criteria with a median age of postnatal ultrasound at 1.6 months (IQR 0.5-3.6). The median (IQR) follow-up time was 7.5 years (4.9-9.2). During time of surgery, 25 (52%) of Wilms patients had contralateral hypertrophy (2 SD above mean), while at diagnosis 9 (24%) of MCDK patients had contralateral hypertrophy, p=0.03. Throughout follow-up contralateral hypertrophy was mostly a consistent finding, although small fluctuation exists (Figure 1). The majority of patients (~50%) with Wilms tumor had contralateral hypertrophy (2 SD above mean) about 1 year after surgery. The majority of patients (~50%) with MCDK had compensatory hypertrophy about 3 years after diagnosis (Figure 2). In the sub-analysis, creatinine clearance was calculated in 70 patients. After adjusting for age, as renal length increases by one centimeter, creatinine clearance increased by 8.2 (95% CI 2.1-14.3, p=0.009).
Conclusions
Contralateral hypertrophy appears to be a compensatory mechanism for unilateral kidney pathology and often occurs at the time of diagnosis. Once a kidney develops hypertrophy, it appears to to be permanent. Renal hypertrophy should be monitored well into adulthood. The theoritical possibility of hyperfiltration injury leading to renal insufficiency was not observed in either the MCDK or Wilms tumor cohort. Renal length can be used as a surrogate for renal health in pediatric patients with solitary kidneys as renal length directly correlates with creatinine clearance.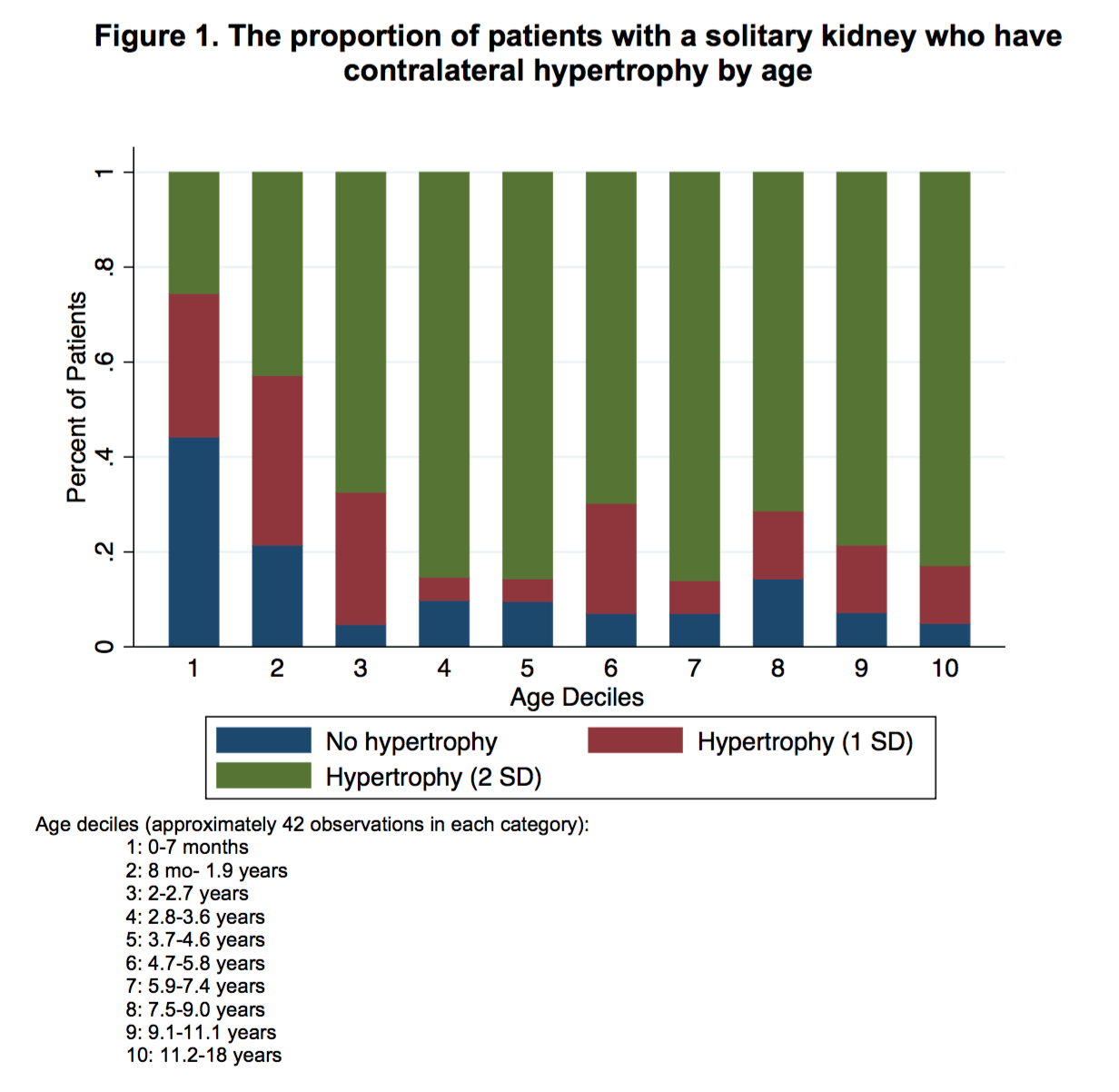
Back to 2017 Program