
Primary Non-Refluxing Megaureter: Analysis of Risk Factors for Spontaneous Resolution and Surgical Intervention
Adriana Dekirmendjian, BHSc1, Mandy Rickard, MN, NP2, Bethany Easterbrook, B.Kin1, Vicki Kam, BHSc1, Melissa McGrath, BHSc1, Natasha Brownrigg, MN, NP2, Jorge E. DeMaria, MD1, Armando J. Lorenzo, MD3, Luis H. Braga, MD, PhD1.
1McMaster University, Hamilton, ON, Canada, 2McMaster Children's Hospital, Hamilton, ON, Canada, 3The Hospital for Sick Children, Toronto, ON, Canada.
Background: The risk of febrile urinary tract infection(fUTI) in primary non-refluxing megaureter(PM) patients has been extensively studied in the literature, however, a paucity of information exists regarding risk factors for surgical intervention and spontaneous resolution. Therefore, we sought to analyze data from our prospective PM cohort to determine risk factors that would predict surgery and resolution in this population.
Methods: Patients with PM were identified from our prospectively collected prenatal hydronephrosis(HN) database from 2008-2016. Primary outcomes included surgical intervention and resolution of ureteral dilation. Resolution was defined as ureteral dilation <7mm at last follow-up. Age at presentation, gender, development of fUTI, HN grade[low(SFU I/II) vs. high(SFU III/IV)], anteroposterior diameter(APD) measurements and ureteral dilation at baseline and last follow-up were recorded. Univariate and multivariable analyses(binary logistic and cox regressions) were performed to identify risk factors for surgery and spontaneous resolution.
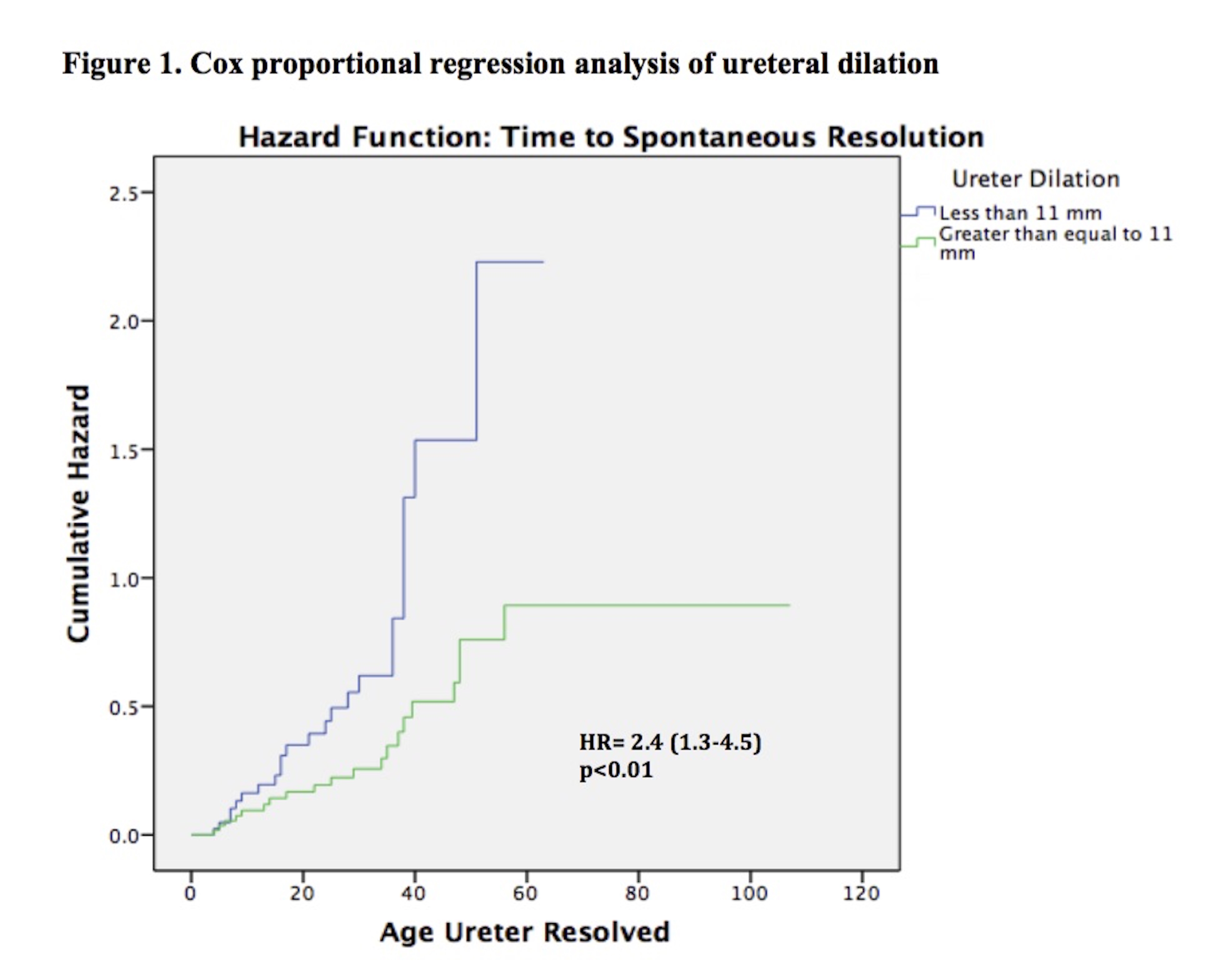
Results: Of 101 patients, 86(85%) were male, and 80(79%) had high grade HN. Median age at baseline and last follow-up were 2(0-23) and 29(2-107) months, respectively. Overall, 23(23%) patients underwent surgery at a median age of 22(3-35) months. Mean ureteral diameter was larger in surgical patients versus those treated non-surgically (14+4mm vs.11+3mm;p<0.01). Of the 78(77%) non-surgical patients, 43(55%) showed resolution of their ureteral dilation at a median age of 24(4-56) months. Survival analysis demonstrated that 12 patients resolved by year 1, 22 by year 2, 30 by year 3, 40 by year 4, and 43 by year 5. However, when considering resolution as APD <10mm, 62(79%) children resolved their HN by last follow-up(29 months). Univariate and multivariable analyses(Table 1) revealed that high-grade HN at baseline, development of fUTI, and ureteric dilation ≥14mm were significant risk factors for surgical intervention. Cox regression(Figure 1) found that ureteral dilation <11mm was the only independent risk factor significantly associated with PM resolution(Table 2).
Conclusion: PM children with high-grade HN, ureteral dilation ≥14mm and fUTI were at a significantly higher risk of undergoing surgical treatment, and those with ureteral dilation <11mm were more likely to resolve spontaneously within 24 months.
Table 1. Univariate and multivariable analysis of risk factors for surgical intervention
| Surgery n=23 (%) | Univariate | Multivariable | ||||
| Total n=101 | p-value | HR (95% CI) | p-value | |||
| Gender Male Female | 20 (23) 3 (20) | 86 15 | 1.00 | Ref 1.4 (0.3-7.2) | 0.67 | |
| HN Grade Low grade (I/II) High grade (III/IV) | 1 (5) 22 (28) | 21 80 | 0.04 | Ref 12.8 (1.3-122.9) | 0.03 | |
| fUTI Yes No | 11 (46) 12 (16) | 24 77 | <0.01 | Ref 7.7 (2.2-26.1) | <0.01 | |
| Ureteral Dilation < 14 mm > 14 mm | 12 (15) 11 (48) | 78 23 | <0.01 | Ref 5.8 (1.8-18.8) | <0.01 | |
Table 2. Univariate and multivariable analysis of risk factors for resolution
| Resolution n= 43(%) | Univariate | Multivariable | ||||
| Total n=101 | p-value | HR (95% CI) | p-value | |||
| Gender Male Female | 36 (42) 7 (47) | 86 15 | 0.73 | Ref 1.2 (0.5-2.7) | 0.69 | |
| HN Grade Low grade (I/II) High grade (III/IV) | 13 (62) 30 (38) | 21 80 | 0.04 | Ref 1.6 (0.8-3.0) | 0.19 | |
| Ureteral Dilation < 11 mm > 11 mm | 23 (53) 20 (34) | 43 58 | 0.06 | Ref 2.4 (1.3-4.5) | <0.01 | |
Back to 2017 Program