
Fast Track Protocol for Cystoscopy and Ureteral Stent Removal in Pediatric Patients
Candace F. Granberg, M.D.1, Carlos Villanueva, M.D.2, Dana Giel, M.D.3, Sean Corbett, M.D.4, Adam Hittelman, M.D.5, Rhys Irvine, M.D.3, Jennifer G. Dwyer, M.D.2, George Chiang, M.D.6, Vijay Vemulakanda, M.D.7, Jonathan Routh, M.D.8, Patricio C. Gargollo, M.D.1.
1Mayo Clinic, Rochester, MN, USA, 2University of Nebraska Medical Center, Omaha, NE, USA, 3UT Le Bonheur Children's Hospital, Memphis, TN, USA, 4University of Virginia Children's Hospital, Charlottesville, VA, USA, 5Yale School of Medicine, New Haven, CT, USA, 6Rady Children's Hospital, San Diego, CA, USA, 7Children's Hospital Colorado, Aurora, CO, USA, 8Duke University Medical Center, Durham, NC, USA.
BACKGROUND: Pediatric surgical centers across the country have widely variable practices regarding anesthesia management for short, minimally-invasive procedures. Institutions may mandate placement of an endotracheal tube (ET) or laryngeal mask airway (LMA) for all cases, some require peripheral IV (PIV) placement for all cases, and some require both. Some institutions also place patients in stirrups in the dorsal lithotomy position on a standard operating table for cystoscopy procedures, which adds to the overall time in the operating room (OR). We sought to compare total OR time and outcomes of cystoscopy and ureteral stent removal in pediatric patients using a "fast-track protocol" consisting of performing the procedure on the patient transport cart in the frog-leg position (Figure 1) with mask/LMA-only anesthesia versus ET/LMA+IV. To date, safety with a fast-track protocol has not been reported.
METHODS: We performed a multi-institutional, retrospective review of patients age 17 years of age and younger who underwent cystoscopy and ureteral stent removal. Exclusion criteria included those undergoing concurrent procedures under the same anesthetic. Patients were divided into two groups: mask or LMA with no IV (Group 1) and ET/LMA+IV (Group 2). Patient demographics, procedure time, and total time in the OR were recorded. Any adverse perioperative events including laryngospasm, conversion from mask to ET/LMA, need for IV placement, or need for IV medication administration in the PACU were documented. Data was analyzed using SAS University Edition.
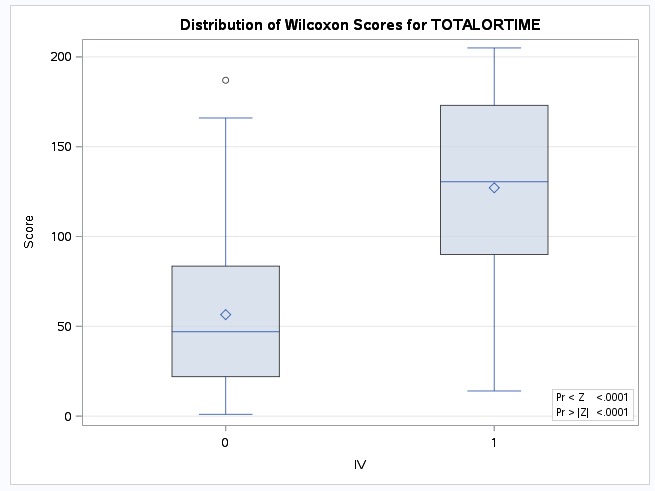
RESULTS: There were 205 patients who underwent cystoscopy and ureteral stent removal at a median age of 45 months (IQR 12-125), with 70 in Group 1 and 135 in Group 2. Age was not significantly different in those who did and did not have IV placed. Median time in OR for Group 1 was 15 minutes (IQR 13-20) versus 25 minutes (IQR 20-31) for Group 2 (p<0.0001). No Group 1 patients experienced laryngospasm, and none required conversion to ET/LMA placement. No Group 1 patients required IV placement in the OR or PACU, thus no patients in Group 1 received any IV medications. CONCLUSIONS: General anesthesia without an IV is safe for short endoscopic procedures such as cystoscopy with ureteral stent removal. Most procedures can be done on the patient cart, eliminating need for transfer to the operating table and use of stirrups. Conversion of these standard anesthesia and patient positioning practices to a fast-track protocol can decrease anesthesia time and overall time in the operating room, thus decreasing costs. Collaboration on a fast-track protocol for these cases in conjunction with pediatric anesthesia should be considered for appropriately selected patients.
Back to 2017 Program