
How To Avoid Scrotoplasty in Boys With a Concealed Webbed Penis: A Preliminary Report on The Paraphimotic Band Technique
Jason P. Van Batavia, MD, David I. Chu, MD, Diana K. Bowen, MD, Mark R. Zaontz, MD.
The Children's Hospital of Philadelphia, Philadelphia, PA, USA.
Introduction:
There are a myriad of techniques to correct concealed penis. Those patients with significant penoscrotal webbing often undergo a scrotoplasty as part of their corrective surgery. This may add time to the surgical procedure and result in scars along the ventral penoscrotal junction. In an attempt to obviate the need for scrotoplasty, we have modified the surgical approach to these patients and report here on our preliminary results. We hypothesized that this technique will lead to minimal post-operative complication with high success rate including good post-operative cosmetic appearance to the penis and scrotum.
Material and methods:
All boys who underwent correction of penile concealment with the presence of significant scrotal webbing using a paraphimotic band incision dorsally and ventrally to avoid scrotoplasty (figure 1A) from July 2014 through May 2017 were registered prospectively into an IRB-approved database. For all patients, any complications, skin infections, and success of surgery (defined as cosmetic appearance with correction of concealment and webbing) were reviewed. The paraphimotic band technique involves retracting the foreskin proximally. This creates a paraphimosis and by incising each band at the 12 and 6 o'clock positions, the scrotal web appears to drop back to a more normal anatomic configuration (see figure 1B-D). The remaining shaft is then degloved and locking sutures are placed at 12, 5, and 7 o'clock at the base of the penis in buck's fascia and affixed to the corresponding dermis of the abdominal wall/shaft skin junction using 4-0 polydioxanone suture (absorbable monofilament) (figure 1E). The shaft skin is then unfurled and excess skin excised with the circumcision defect approximated with chromic catgut.
Results:
Overall, 71 consecutive boys underwent the paraphimotic band technique. Median age at time of surgery was 8 months (interquartile range [IQR]= 7-14.3months) and median follow up was 3.1 months (IQR = 1-6months; mean=4.0months). All patients had excellent penile shaft exposure with no significant webbing noted (figure 1F). Four patients (6%) had very mild concealment secondary to large mons pubis fat pads. There were two post-operative complications (2.8%) including a superficial skin infection requiring oral antibiotics (Clavien 2) in one boy and post-operative bleeding requiring emergency room visit, manual pressure and reapplication of dressing (Clavien 1) in another boy. Two boys (2.8%) complained of dysuria for 2-3days after surgery that resolved spontaneously.
Conclusions:
The paraphimotic band modification for reconstruction of the concealed penis is easy to perform and appears to be successful and reproducible in the short term. In addition, this technique avoids the need for scrotoplasty in cases of penile webbing and concealment. Most scrotoplasty techniques result in scars along the ventral penoscrotal junction and therefore the paraphimotic band technique may result in improved cosmesis. Minor (Clavien grades1-2) complications are rare but can occur as with any penile surgery. Despite excellent early cosmetic appearance, further follow-up is necessary to confirm that this procedure stands the test of time.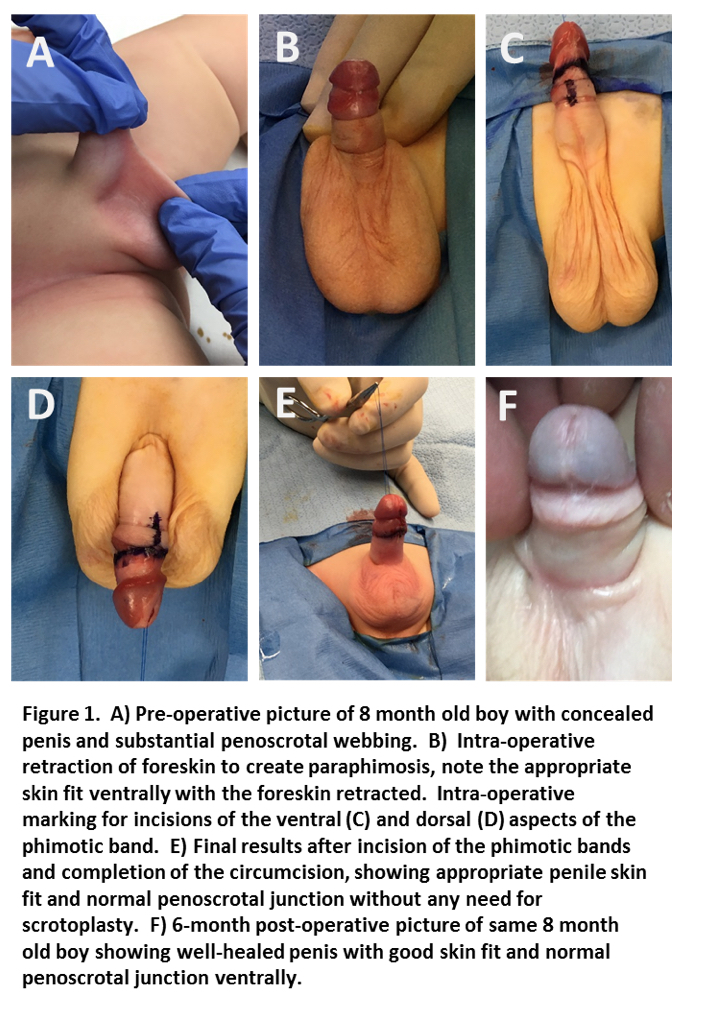
Back to 2017 Program