-->
|
Back to 2014 Fall Congress Meeting Abstracts
Presentation and Outcomes of Renal Cell Carcinoma (RCC) in Children, Adolescents and Young Adults: a National Cancer Database Study
Ardavan Akhavan, MD, Morgan Richards, MD, Adam Goldin, MD, MPH, Kenneth Gow, MD, MPH, Paul A. Merguerian, MD.
Seattle Children's Hospital, Seattle, WA, USA.
BACKGROUND:
RCC rarely occurs in the pediatric population. Outcomes have been limited to several small case series. We queried a large national cancer database to describe presentation and outcomes and determine risk factors associated with mortality in children presenting with RCC and compared them to adolescents and young adults. We hypothesize that younger patients present with more advanced disease, and mortality is associated with pathological subtype and stage.
METHODS:
We queried the National Cancer Database for patients 30 years and younger with RCC, from 1998 - 2011. Patients were then divided into 3 age groups: under 15, 15 -21 and 21-30 years. Demographic parameters, cancer subtype and stage, treatment, and mortality were compared between groups. Univariate analysis was performed to determine significant factors. Survival was analyzed using Cox regression, controlling for age, stage, tumor subtype, insurance status, race, regional population, and type of first line therapy.
RESULTS:
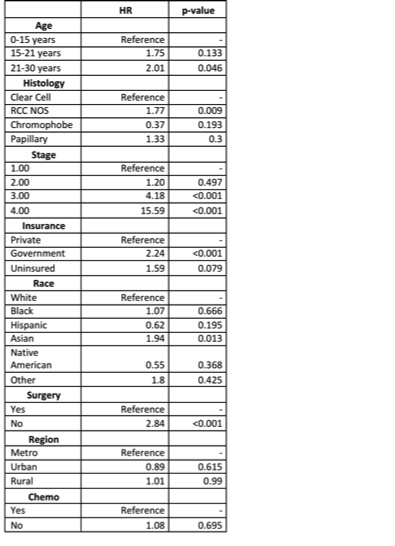
A total of 3,558 patients were available for analysis. Of these, 161 were <15 years and 337 were 15 - 21years. While there were more males in the <15 age group (p=0.046), there were no other significant differences in demographic variables between patients in the different age groups. Younger patients presented with higher stage (p<0.001), higher grade (p<0.001), and larger tumors (p<0.001). A higher proportion of RCC Not Otherwise Specified (NOS) and papillary histologies (p<0.001) were found in the younger patients. Additionally, younger patients had a higher proportion of positive lymph nodes (p=0.006). There was no significant difference in the proportion of patients who underwent surgery between the age groups (p=0.464); however, a significantly higher percentage of younger patients underwent lymph node resection (p<0.0001) and received chemotherapy (p<0.0001). Cox regression controlling for age, stage, histology, insurance, race, regional population, and type of first treatment demonstrated that age 21-30 years, RCC NOS histology, stage 3-4, Asian race, government insurance, and not undergoing surgery as first line therapy were all associated with increased mortality (Table I).
CONCLUSIONS:
Children and adolescents present with more advanced disease and different prevalence of histological subtypes than young adults. Higher mortality in young patients may be associated with older age, RCC NOS histology, higher stage, Asian race, government insurance, and not undergoing surgery as a first line therapy. Further studies are necessary to validate these findings.
Back to 2014 Fall Congress Meeting Abstracts
|

