-->
|
Back to 2014 Fall Congress Meeting Posters
Clean-Intermittent Catheterization as an Initial Management Strategy Provides for Adequate Preservation of Renal Function in Patients with Persistent Cloaca
David J. Chalmers, MD1, Kyle O. Rove, MD2, Cole A. Weidel, MD2, Suhong Tong, PhD1, Georgette L. Siparsky, PhD1, Duncan T. Wilcox, MD1.
1Children's Hospital Colorado, Aurora, CO, USA, 2University of Colorado, Anschutz Medical Campus, Aurora, CO, USA.
Background
Persistent cloaca is a rare, congenital anomaly involving the genital, urinary and rectal organ systems. Bladder outlet obstruction and hydrometrocolpos can lead to obstructive uropathy, abdominal distention, infection, perforation and acidosis. Management strategies include early surgical diversion (vesicostomy, vaginostomy, nephrostomy) and clean-intermittent catheterization (CIC) of the common channel. We hypothesized that CIC is an adequate means of genitourinary decompression, regardless of the severity of cloacal anomaly.
Methods
We reviewed all patients with persistent cloaca from a single center from 1995 to 2013. Abstracted data included renal function (baseline GFR and serial creatinine prior to definitive reconstruction), presence of hydrocolpos, hydronephrosis, vesicoureteral reflux (VUR) or renal dysplasia, and common channel length. A linear mixed model was used to calculate creatinine change over time in relation to management strategy. Estimated GFR was calculated using the Schwartz equation for neonates. T-test was used for continuous data and Fisher’s exact test was used for binomial data. P<0.05 was considered significant.
Results
25 patients were identified. 9 (36%) underwent surgical diversion vs 16 (64%) managed by CIC. 7 had short common channels (< 3cm) vs 18 with long common channels (≥ 3cm). 22 patients had serum creatinine data available for analysis. There was no significant difference in hydronephrosis, high-grade hydronephrosis (grades III-IV, p=0.62), any VUR (p=0.33), high-grade VUR (grades III-V, p=0.62), hydrocolpos (p=0.21) or renal dysplasia (p=0.42). No significant differences were found between baseline GFR for diversion (16.8 mL/min per 1.73 m2) versus CIC (28.7 mL/min per 1.73 m2, p=0.22). There was no difference in creatinine trend (See Figure).
Conclusions
CIC is an adequate initial management strategy to decompress the genitourinary tract in patients with persistent cloaca. CIC preserves renal function similar to early surgical decompression. 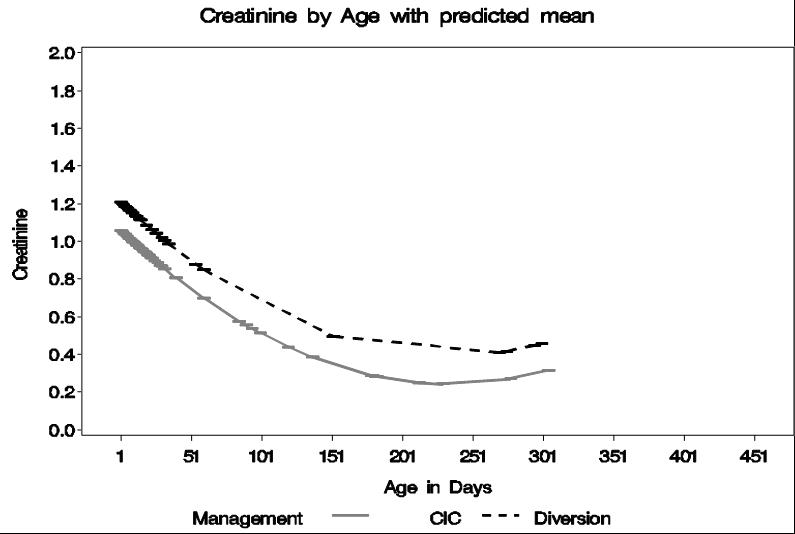
Back to 2014 Fall Congress Meeting Posters
|

