
The Need for Reoperations in Patients Undergoing Outpatient Distal Hypospadias Repairs in a Large, Multi-State Cohort
Yuri Sebasti�o, PhD, Christopher T. Brown, MD, Jennifer Cooper, PhD, Daryl J. McLeod, MD, Daniel DaJusta, MD.
Nationwide Children's Hospital, Columbus, OH, USA.
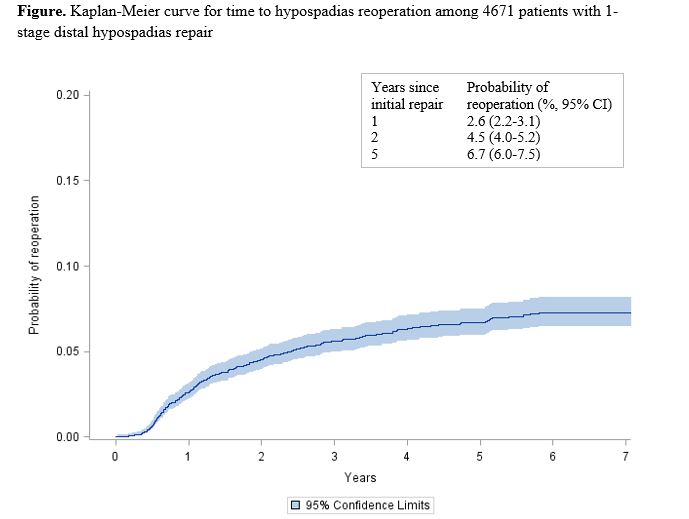
Background: Hypospadias is one of the most common congenital urologic anomalies in the United States. In families that chose surgery, most children undergo hypospadias repair before 2 years of age. Despite increases in the use of outpatient surgical repair, the risk of post-surgical complications is seldom reported outside of academic or tertiary center studies, many of which are single-institution based with <2 years of median patient follow-up time. Furthermore, the complication rate following repair of distal defects has not been evaluated in a representative, nationwide sample. We examined the rates of additional surgical interventions for complications following outpatient distal hypospadias repair in a large, representative population of U.S. children. Methods: We conducted a retrospective cohort study of pediatric patients with hypospadias and 1-stage distal hypospadias repair using State Ambulatory Surgery and Services Databases from 10 states. The databases allow tracking individual patients’ encounters over time across all or nearly all ambulatory surgical centers within each state. Patients who underwent ambulatory surgery in 2008-2013 were identified using Current Procedural Terminology (CPT) codes. Patients with records suggesting multiple 1-stage repairs, prior surgery for hypospadias complications, or with <2 years of follow-up were excluded. Reoperations following the 1-stage repair were identified by searching for return ambulatory surgery encounters with CPT codes for open surgical treatment of hypospadias complications (including fistula, diverticulum and stricture) in 2008-2015. Follow-up time was defined as time from initial repair to first reoperation or last month of data available (for patients without reoperation). Time-to-event analyses (Kaplan-Meier and proportional hazards regression) were used to estimate the risk of reoperation over time and to identify patient sociodemographic and surgical facility characteristics predictive of reoperation. Results: A total of 4671 children treated across 156 institutions were included. The median follow-up time was 4.1 years (range 2-7.9). Most patients were <2 years of age at the time of their hypospadias repair (53.2% infants, 26.4% age 1). The estimated risk of having a reoperation within five years after repair was 6.7% (95% Confidence Interval: (CI) 6.0-7.5%; Figure). About 14.5% of patients who had a reoperation did so at a different institution than the initial repair. Patients aged 2-3 years at the time of repair were 45% more likely to have a reoperation compared to infants (hazard ratio: 1.45; 95% CI: 1.02-2.04; P=0.036). No other factors evaluated had a significant association with risk of reoperation. Conclusions: Approximately 7 out of 100 children undergoing 1-stage distal hypospadias repair are expected to have a reoperation for complications within 5 years. These findings contribute to a broader understanding of the risk of reoperations following distal hypospadias repair. Future work should examine reasons for apparent increased risk of reoperation for children aged 2-3 years compared to infants.
Back to 2018 Program



