
An SPU survey of opioid prescribing practices after ambulatory pediatric urology procedures
Jennifer J. Ahn, MD, MS, Jonathan S. Ellison, MD, Paul A. Merguerian, MD, MS.
Seattle Children's Hospital, Seattle, WA, USA.
Introduction: The crisis of opioid dependence and abuse is a national Public Health Emergency and overprescribing of opioids has been identified as a significant driving factor. Evidence suggests that adult surgical patients use far less medication than prescribed, leading to potential misuse or accidental ingestion, though prescription patterns in the pediatric surgical population are not well described. In this study, we sought to assess pediatric urologists’ practice patterns in prescribing opioids for routine outpatient procedures. We hypothesized that prescribing practices vary widely across North America.
Methods: After obtaining IRB approval, members of the Society of Pediatric Urology were e-mailed an invitation to participate in a 23-question survey. Eight clinical vignettes were used to assess type and duration of opioid prescriptions in multiple choice format. Respondent characteristics and attitudes towards opioid prescription were also assessed. Reminders were sent at two and four weeks. All survey responses were anonymous and stored in REDCap. Data were analyzed using descriptive statistics, Fisher’s exact and chi-squared tests. A p-value <0.05 was considered significant. Stata 14 and Microsoft Excel were used for all analyses.
Results: A total of 102 responses were received with a response rate of 31%. Fourteen percent of respondents reported giving no opioids for all of the procedures, while 48% (49/102) give opioids for all cases described (Figure 1). Half of respondents routinely prescribe opioids for 8 month-olds weighing 9kg undergoing circumcision, hernia repair, or orchiopexy. Longer prescription duration was associated with older age (p < 0.001) but not with surgery type. Acetaminophen-hydrocodone was the opioid most commonly prescribed (57%), followed by oxycodone (28%) and acetaminophen-oxycodone (11%). Three respondents (3%) reported prescribing acetaminophen-codeine, despite the FDA’s black box warnings.
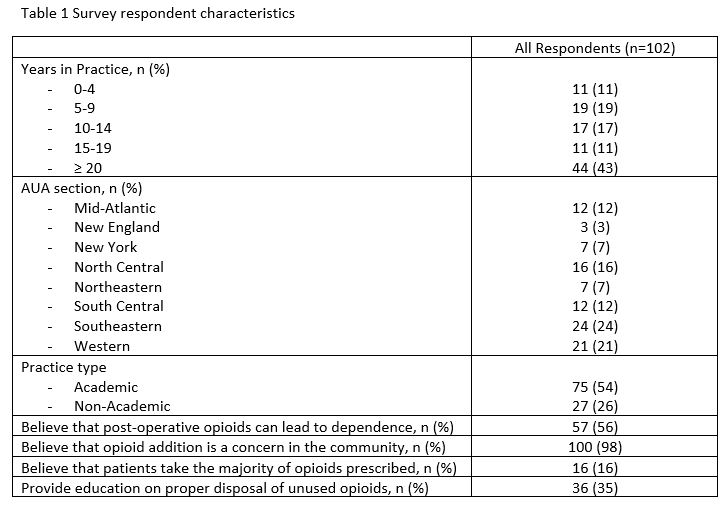
Respondents primarily work in academic settings, and all AUA sections were represented (Table 1). The vast majority (98%) agree that addiction is a concern in their community, while only 56% believe that post-operative opioid administration can lead to dependence. Only 35% provide education to patients on proper disposal of unused opioids, and only 16% believe patients take the majority of given opioids. The total number of procedures for which opioids are prescribed was associated with AUA section, with 69% of North Central section respondents and 67% of Southeastern section respondents prescribing opioids for all 8 procedures (p = 0.003). Use of acetaminophen-hydrocodone and oxycodone was associated with more frequent prescribing (p=0.003). Prescribing practices were not associated with practice type, attitudes and beliefs, or years in practice.
Conclusion: Opioid prescribing practices after ambulatory pediatric urology procedures vary significantly by provider and region. Many respondents prescribe no opioids, suggesting that many pediatric urologists may overprescribe opioids for routine surgery. Given these findings, decreasing prescriptions and implementing education on proper disposal are potential areas for immediate intervention. 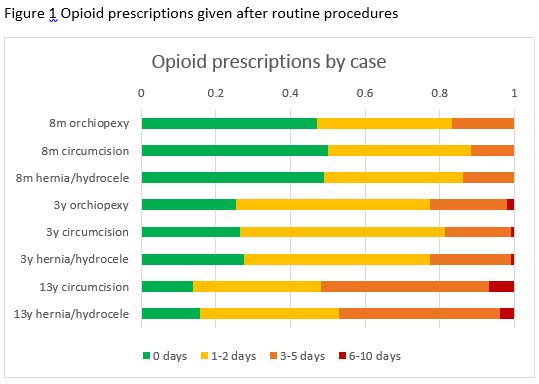
Back to 2018 Program



