
Inverted Kidney: Single Center Experience with “Upside Down” Positioning of Renal Allograft During Pediatric Transplantation
Mandy RIckard, MN, NP, Nicolas Fernandez, MD, Anne-Sophie Blais, MD, Martin A. Koyle, MD, Katherine Taylor, MD, Smruthi Ramesh, MD, Armando J. Lorenzo, MD, MSc.
Hospital for Sick Children, Toronto, ON, Canada.
Introduction:
For structural reasons during transplantation the allograft is preferentially transplanted into the right iliac fossa, therefore an allograft with vascular anatomical variants (such as a short renal vein), may pose a challenge. As an option, the donor kidney may be placed in an inverted fashion in order to establish a more straightforward anastomosis for the vessels. Herein, we reviewed our experience of inverted renal transplants in pediatric patients with at least 1 year of follow up.
Methods:
We reviewed all patients having a renal transplant between January 2012 and December 2016. We identified children who underwent an inverted renal transplant and extracted perioperative and postoperative data. Because all inverted transplants were from deceased donors, living donor transplants were excluded. Inverted positioning of the allograft in the flank and pelvic cavity is as demonstrated in Figure 1. We defined early graft function as the time to reach creatinine nadir and patients were censored at time of last follow up.
Results:
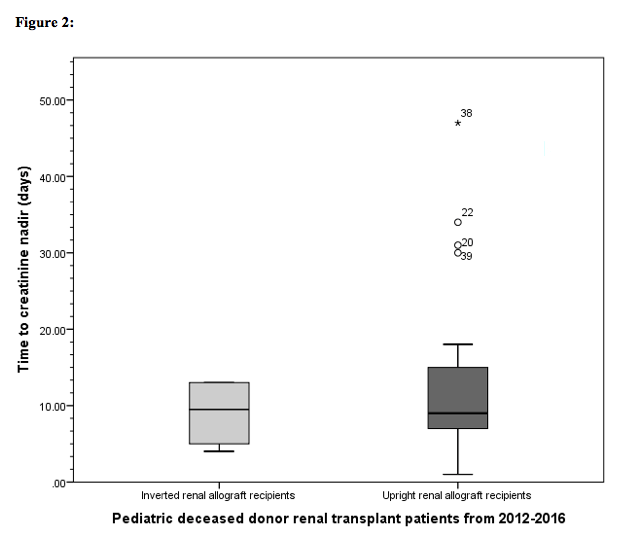
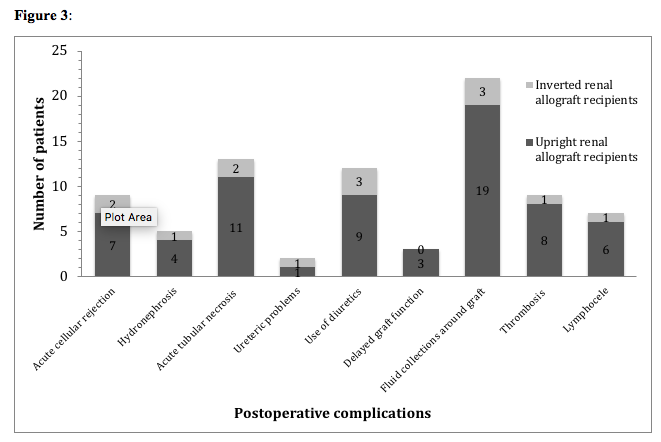
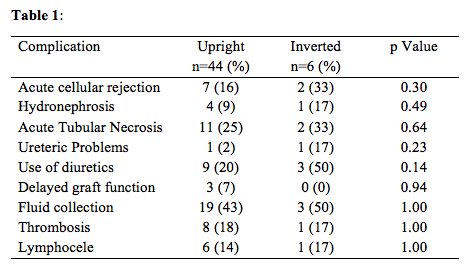
Of 81 transplants, 50 (62%) were from deceased donors and 6(12%) received inverted renal grafts. Half (3/6) were female, 5/6 (83%) were dialysis dependent, 5/6 received right allografts and preoperative serum creatinine was 766.3 μmol/L-1 (range 438-1500 μmol/L1). Weight at surgery was 35 kg (15.6-56.3), median age was 13 years (4-17) and follow-up was 36.6 months. The common iliac artery was the anastomosis site for 50% of the patients, the external iliac for 33.3% and the aorta in 1 patient. The vena cava was the anastomosis site for 50% of the patients, the external iliac for 33.3%, and the common iliac for one patient. End-to-side ureteroureterostomy was performed in 5/6 patients with ureteroneocystotomy in the other. There was no difference in time to creatinine nadir of the upright group (12+9days) vs. the inverted group (9+4days) (p=0.43) (Figure 2). We also found no significant differences in the rates of post-operative complications between children who received upright vs. inverted allografts (Figure 3/Table 1).
Conclusion:
Inversion of renal allografts (i.e. “upside-down” kidney) in pediatric patients is a viable surgical technique to compensate for shortcomings in anatomy or in special cases of renal transplantation involving a short donor renal vein. Future research in this field should focus on the outcomes of a larger group of pediatric transplant recipients with inverted allografts to lend support to the suitability and safety of this procedure in this patient population.
Right flank/iliac fossa 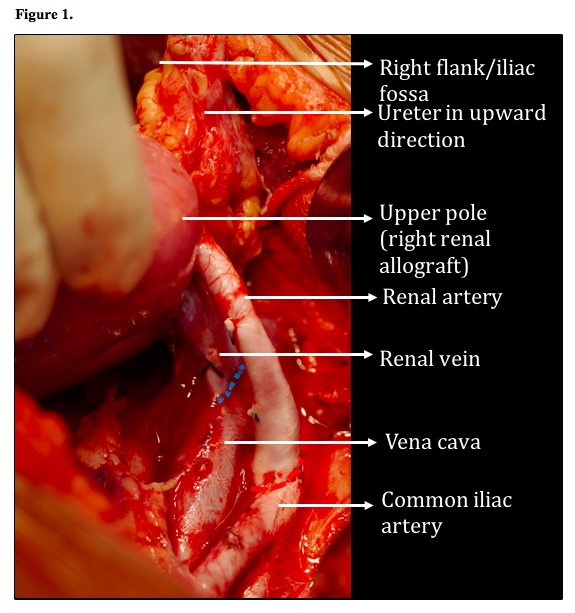
Back to 2018 Program



