
Distance between trocars, remote centre location and surgical field in robot-asssited pediatric surgery: a critical triad for optimal Si robot functionality.
Nicolas Fernandez, M.D., PhD1, Austin Morgan, BS2, Pan Zouxin, BS2, Jessica Ming, M.D.3, Thomas Looi, PhD2, Walid Farhat, M.D.4.
1Hospital Universitario San Ignacio Pontificia Universidad Javeriana, Bogota, Colombia, 2Hospital for SickKids, Toronto, ON, Canada, 3University of New Mexico, Albuquerque, NM, USA, 4Hospital Universitario San Ignacio Pontificia Universidad Javeriana, Toronto, ON, Canada.
Introduction:
Robot-assisted laparoscopic surgery has become widely prominent in pediatric surgery. Instrument size and small working space are current technical challenges. Our aim is to examine the impact of trocar insertion spacing and depth on the effective intra-abdominal working space (EWS).
Methods:
After Animal Care Committee approval, we simulated intraoperative robot-assisted surgical scenarios on small porcine models and a 3-D inanimate silicone model (DragonSkin30 by Smooth-On, PA, USA. Shore Hardness 30A, Tensile Strength 500PSI and 100% Modulus 86PSI) for 8, 6 and 4-cm between trocars (Figure 1). Depth of trocar was positioned at 2.5 (remote center (RC)) and 1-cm deep with standard trocars and bariatric ones (1 cm and at RC). Radial measurements of the farthest and nearest functional point for instrument reach were recorded establishing the EWS in both models. Intra-abdominal reach by quadrants was simulated with 3-D silicone model (Figure 2).
Results:
At 8-cm distance, reduction from 2,5 to 1-cm decreases the EWS. For 6-cm, the intra-abdominal mean area of coverage at 2.5 cm was 291 cm2 (SD + 12.7 cm2) vs 183 cm2 (SD + 11.2 cm2) at 1 cm deep (p<0.0000). (Figure 3). For 4-cm distance, the area of coverage did not seem to change significantly but it was reduced compared to 6 and 8-cm. Results between animal and 3-D silicone model are comparable. For bariatric trocars, the area of coverage was similar as with regular ones, but at 1 cm deep the instrument clashing was less at 4 cm distance between ports.
Conclusions:
Reduction in distance between ports and its depth, impacts EWS. A 4-cm distance may be sufficient if the surgical area is located within the EWS. Multi-quadrant surgery might be feasible for trocars at RC with 6 cm distance between ports. A balance between these variables needs to be further evaluated so robot-assisted surgery could be extended not only to small age groups but also for multi-quadrant procedures. Usage of 3-D inanimate model is supported due to similar results as with the animal model.
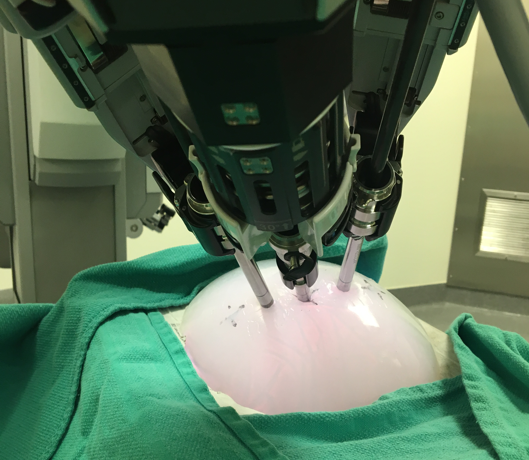
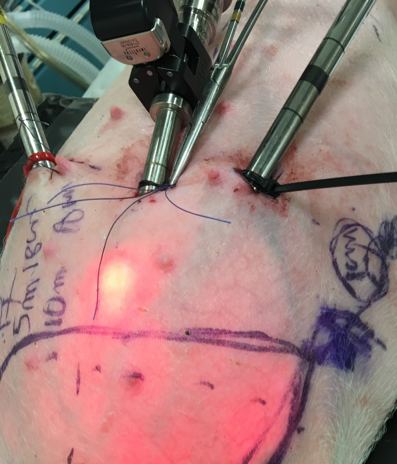
Figure 1. Animal model at 4 cm distance between ports using bariatric ports at 1 cm deep. Figure 2. A 3-D inanimate model for simulation and measurement of intra-abdominal reach measurement to establish intracorporeal EWS.
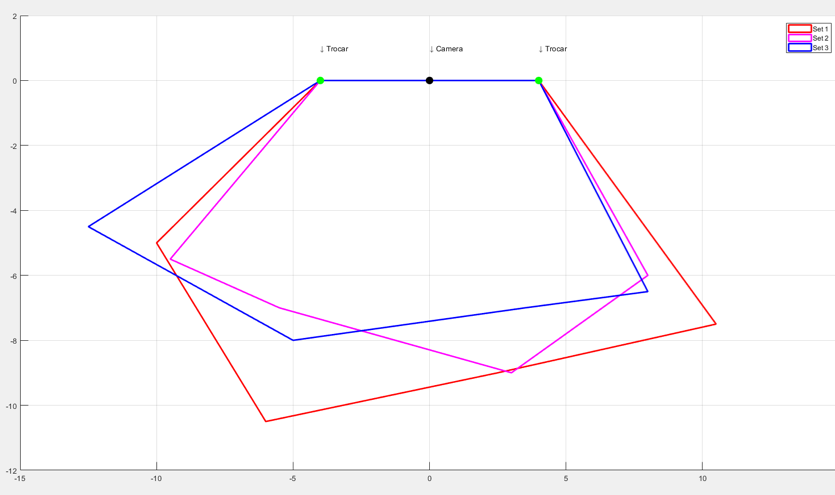
Figure 3. Graphic representation of the area of coverage for intraabdominal coverage. In pink instrument reach with trocar at 1 cm deep and 6 cm distance between ports. In red and blue instrument reach 2.5 cm deep.
Back to 2018 Program



