
Machine Learning of Videourodynamics to Risk Stratify Spina Bifida Patients
Shuvro De, MD, Duncan Smart, BS, Jackson Cabo, BS, Abby S. Taylor, MD, John W. Brock, III, MD, Mark C. Adams, MD, John C. Pope, IV, MD, John C. Thomas, MD, Stacy Tanaka, MD, Chevis Shannon, MBA, MPH, DrPH, MERC, Douglass B. Clayton, MD.
Monroe Carell Jr. Children's Hospital at Vanderbilt University Medical Center, Nashville, TN, USA.
BACKGROUND
Videourodynamic studies (VUDS) are essential in the longitudinal monitoring of spina bifida patients to prevent renal deterioration. Recent studies and large multicenter trials have highlighted the variability in VUDS interpretation among pediatric urologists. We have previously presented our pilot study with a computerized assessment of videourodynamics in the newborn population. In this study, we aimed to expand and validate this assessment to risk stratify all spina bifida patients.
METHODS
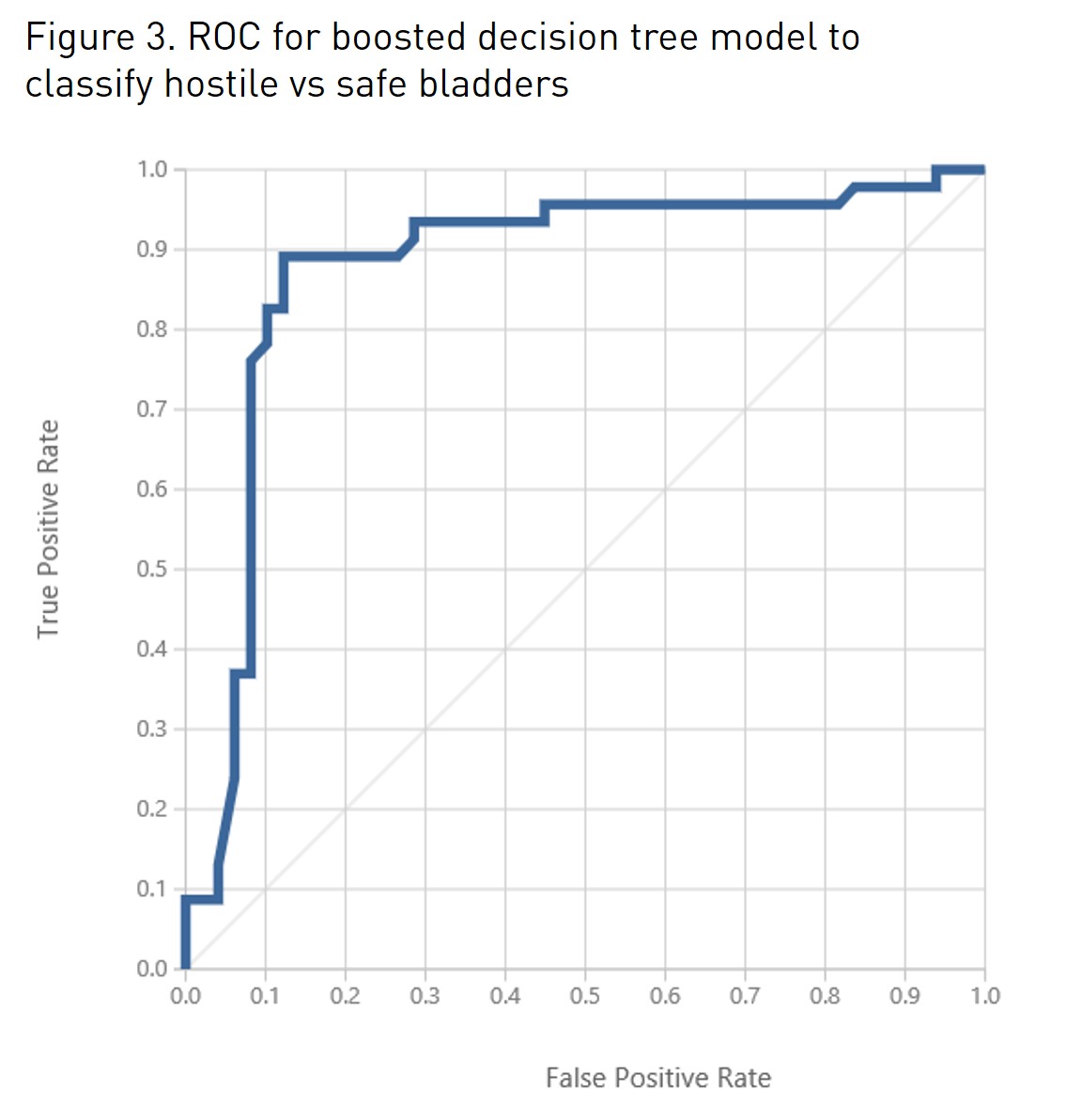
From 2015 to 2018, we identified spina bifida patients and collected raw data from the VUDS. We objectively extracted the following VUDS features: compliance, bladder capacity, detrusor leak point pressure (DLPP) or end-fill pressure (EFP), bladder stress, dynamic pressure changes, and EMG synergy. To evaluate bladder stress, we calculated the area under the curve of the detrusor pressure tracing (AUC-Pdet). To calculate compliance, we calculated linear regression. To evaluate dynamic pressure changes and EMG synergy, we applied Microsoft AzureⓇ Time Series Anomaly Detection, an algorithm used to detect dynamic changes in time series data. All parameters were then normalized to bladder capacity. For each VUDS study, we developed “safe ” versus “hostile ” bladder binary classification defined by development or worsening of trabeculations, hydronephrosis, reflux, or subjective worsening of subsequent UDS tracings within 3 years of the study. Presence of any of these criteria was classified as “hostile” bladder. Absence of all criteria was classified a “safe” bladder. We then applied predictive modeling with two-class boosted decision tree classification with 10-fold cross validation, repeated 100 times, using Microsoft AzureⓇ.
RESULTS
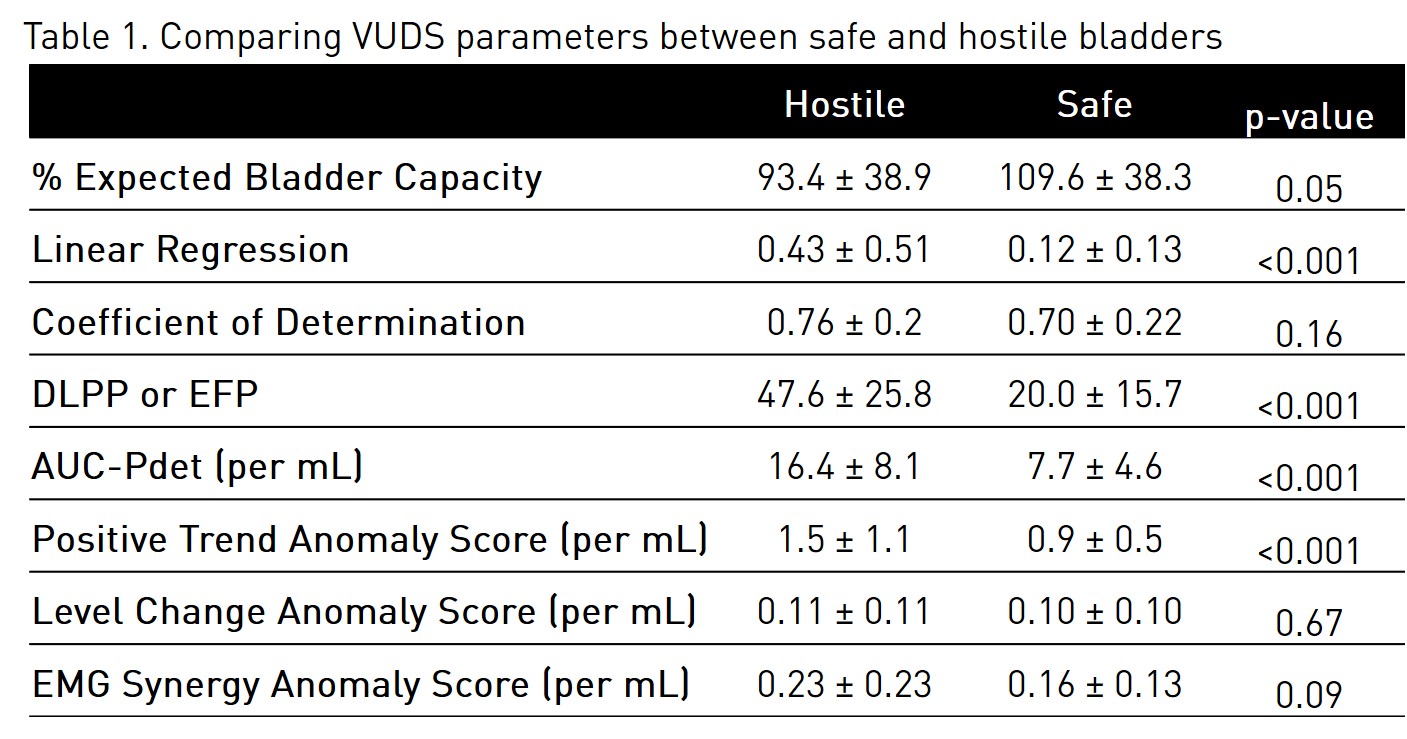
We identified 42 MMC patients, from which 102 VUDS studies were extracted. Seven VUDS studies were excluded due to prior bladder reconstruction or inability to interpret the study. Mean age at time of UDS study was 4.1 ± 4.0 years with a mean follow-up of 23.2 ± 8.6 months. Of the 42 patients, 20 (48%) were female. On chart review, of the 95 VUDS studies analyzed, 46 were identified as hostile bladders based on pre-defined criteria. When comparing safe and hostile bladders, a significant difference was seen in DLPP/EFP, linear regression slope, AUC-Pdet, and Positive Trend Anomaly Score (Table 1). Predictive modeling using two-class boosted decision tree classification predicted clinical progression with an accuracy of 88% (Figure 1). In comparison, using only DLPP/EFP>40 cm H20 revealed a predictive accuracy of 75% in predicting bladder progression.
CONCLUSION
In this study, we developed an objective computerized assessment of VUDS tracings. We then applied machine learning to create an accurate predictive model to classify safe and hostile bladders. In addition, we identified a novel VUDS parameter, AUC-Pdet, that can be implemented in clinical practice and serve as an objective clinical parameter to aid in VUDS interpretation.
Back to 2018 Program



