
CLOSE MONITORING IN THE FIRST YEAR AFTER HYPOSPADIAS REPAIR RESULTS IN EARLY DETECTION OF URETHROCUTANEOUS FISTULAS (UCFs)
Melissa McGrath, BASc1, Hark Randhawa, MD1, Melise Keays, MD2, Smruthi Ramesh, BHSc1, Luis H. Braga, MD PhD1.
1McMaster University, Hamilton, ON, Canada, 2Childrens Hospital Of Eastern Ontario, Ottawa, ON, Canada.
BACKGROUND: Urethrocutaneous fistulas(UCFs)are the most common complications reported post-tubularized incised plate(TIP) urethroplasty. Previous studies have stated that 64% of complications occur at the first post-operative visit(6 weeks)and 80% within the first year. However, a recent publication has found a median time to complication of 1.2 years with patients presenting with urethroplasty related problems up to 3 years post operatively. We hypothesize that the majority of UCFs would occur within the first 6 months post-surgery and that fistulas that were detected immediately after their occurrence (within a week post-catheter removal) could be potentially managed non-surgically with reinsertion of a bladder catheter.
METHODS: Of a prospectively collected hypospadias database(n=733), consecutive TIP repairs from 2008-2019 were selected. Staged repairs, other techniques and redo cases were excluded(n=303). Primary outcome was time to UCF. Age at repair, follow up duration, meatal location, VC before and after degloving, preoperative testosterone stimulation(PTS), type of anesthetic block (caudal vs. dorsal penile block [DPB]) and time to UCF were recorded. Follow up schedule in the 1st year post-repair involved catheter removal at 1 week, clinic visits at 6-8 weeks, 6 and 12 months. In addition, photograph check-ins were done every 3 days over the first 4 weeks postop by a nurse practitioner/hypospadias parent advocate. Time to complication was analyzed using KM curves. Mean time to UCF detection was compared between patients with PTS vs those without, those who had caudal vs. DPB, those with distal vs proximal hypospadias and boys with VC>30 vs <30, using independent t tests.
RESULTS: Of 430 patients, 307(71%) had distal, 76(18%) midshaft and 47 (11%)proximal hypospadias. Median age at surgery was 15.6(13-20.7) months and mean follow-up was 20±22 months. A total of 32(7.4%) UCFs were identified with a median time to UCF of 6.3 months(IQR:1.2-26.2). In 5(16%) patients, whose UCFs developed within a week post-catheter removal, a bladder catheter was reinserted for an additional 7-10 days. All these 5 fistulas resolved spontaneously once the catheter was removed, leaving 27 to be managed surgically. UCFs were detected in 14 patients(52%) by 6 months, in 18(67%) by 12 months, and in 27(100%) by 39 months(Figure 1). We found a difference in mean time to detection of UCF in patients with and without PTS(6.6±3.3 vs 17.7±4.1 mos, p=0.05)and those with a caudal vs DPB(11.8±13.2 vs. 20.9±25.4 mos, p=0.05). Mean time to UCF detection was similar for those with distal vs midshaft/proximal defects(13.9±15.8 vs 12.±15 mos, p=0.83), and for those with VC >30 vs <30(10.3±16.7 vs 13±15.4 mos, p=0.70). Multivariable analysis found no significant association.
CONCLUSION: We observed that 52% of UCFs were detected by a median time of 6 months and that 2/3 of them were detected by 12 months post-hypospadias repair. An active surveillance protocol with photograph check-ins in the 1st month after catheter removal results in earlier UCF detection and may allow some of these fistulas to close spontaneously. 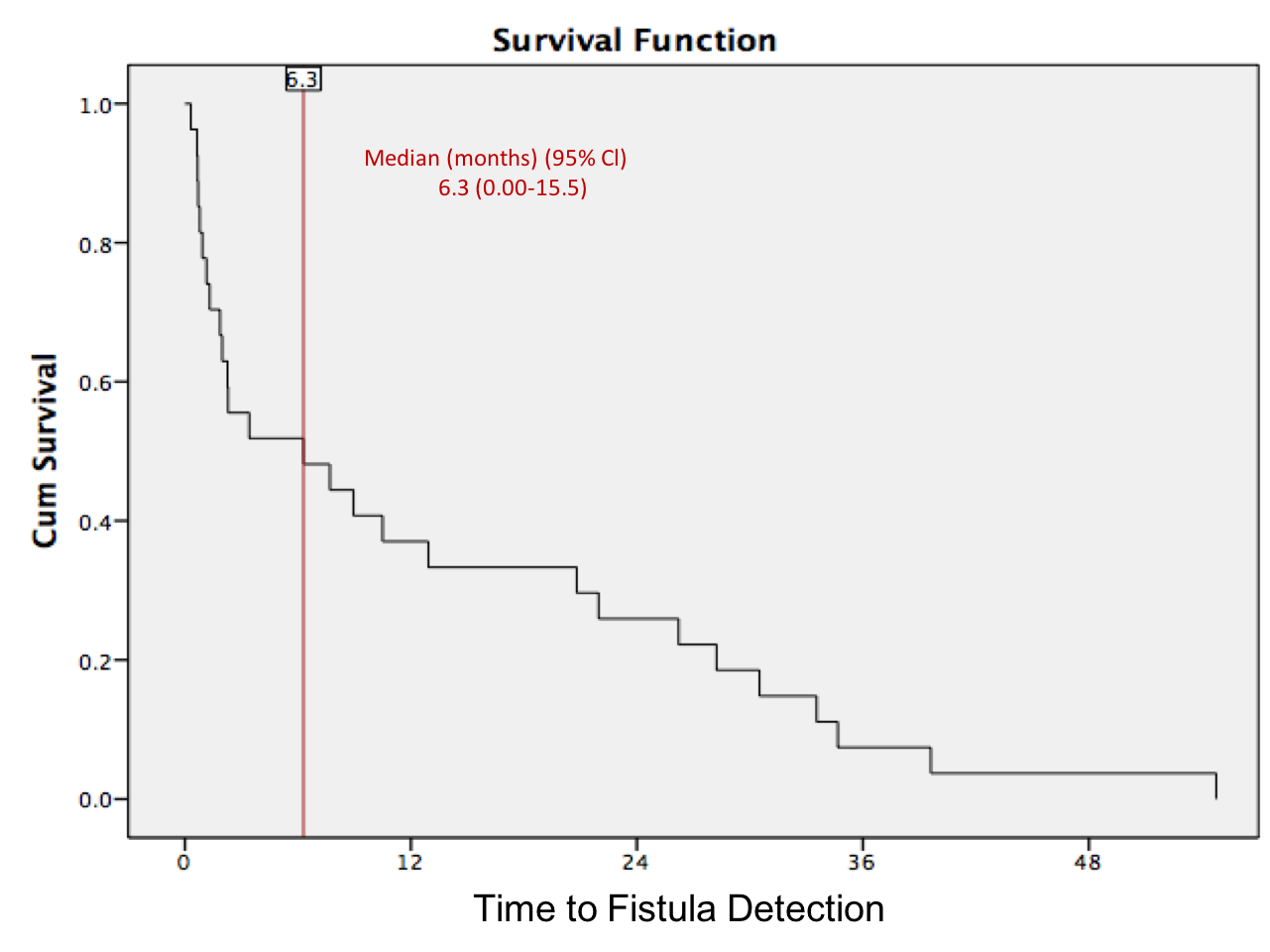
Back to 2019 Abstracts



