
Anxiety, Distress, and Pain in Pediatric Urodynamics
Julia B. Finkelstein, MD, MPH, Dylan Cahill, BA, Kelsey Graber, MS, Kelsey Tulley, CCLS, Brianna O'Connell, MS, CCLS, Lauren Mednick, PhD, Peter Weinstock, MD, PhD, Carlos Estrada, MD, MBA.
Boston Children's Hospital, Boston, MA, USA.
BACKGROUND: Urodynamics (UDS) testing is an invasive procedure commonly used to evaluate lower urinary tract function. To obtain the best possible results, patients are typically kept awake and interactive throughout testing. Naturally, children commonly experience physical and emotional discomfort while undergoing this procedure. We sought to systematically evaluate the pediatric patient UDS experience.
METHODS: We performed a prospective study of patients aged five and older undergoing UDS over a six-month period. Upon arrival at the UDS clinic, caregivers were asked to complete a demographics questionnaire and patients a visual analog scale for anxiety (VAS-A) about the upcoming procedure. A research assistant (RA) observed all UDS studies, including those with an external urethral sphincter needle EMG. The RA assessed the patient's behavior during each major step of UDS using a validated observational measurement method, the brief behavioral distress scale (BBDS). Nursing staff also obtained patients' pain ratings using the Faces (<8 years) or numeric (8+ years) pain scale (0-10) for these key steps. Immediately after UDS, each patient completed a post-test VAS-A along with a brief investigator-developed survey about the UDS experience.
RESULTS: 76 UDS were observed, with almost half (35/76) including needle EMG. The average patient age was 11.6 years and 49% of patients were completely sensate (Table 1). 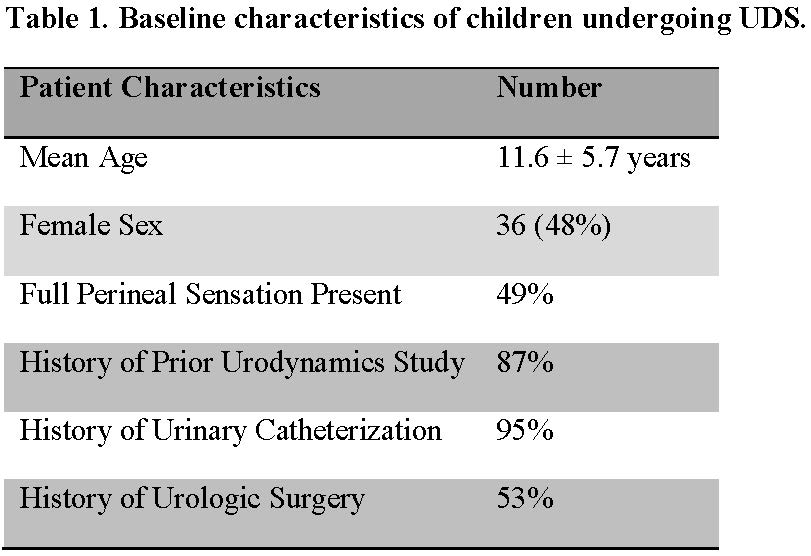
Average patient VAS-A scores were 2.3 out of 10 prior to UDS, compared to 0.8 after testing. Though all patients completed testing, 43% demonstrated interfering or potentially interfering behaviors at some point during the procedure. The highest proportion of interfering and potentially interfering behaviors were observed during EMG needle insertion (31%) and urethral catheter insertion (29%), in agreement with the highest average pain scores of 3.2 and 2.7, respectively. 18% of patients exhibited behavioral distress after being asked to void, which took a median of 5 minutes (IQR 0-7.8) to initiate. Fewer than half of patients (46%) reported being completely aware of what was going to happen before the procedure and 27% of patients noted that something unexpected or surprising happened during testing. After excluding those who reported being completely aware of what to expect, 50% of patients had at least one interfering or potentially interfering behavior (Table 2). Similarly, of those who had no prior history of UDS, 60% of patients had at least one interfering or potentially interfering behavior. 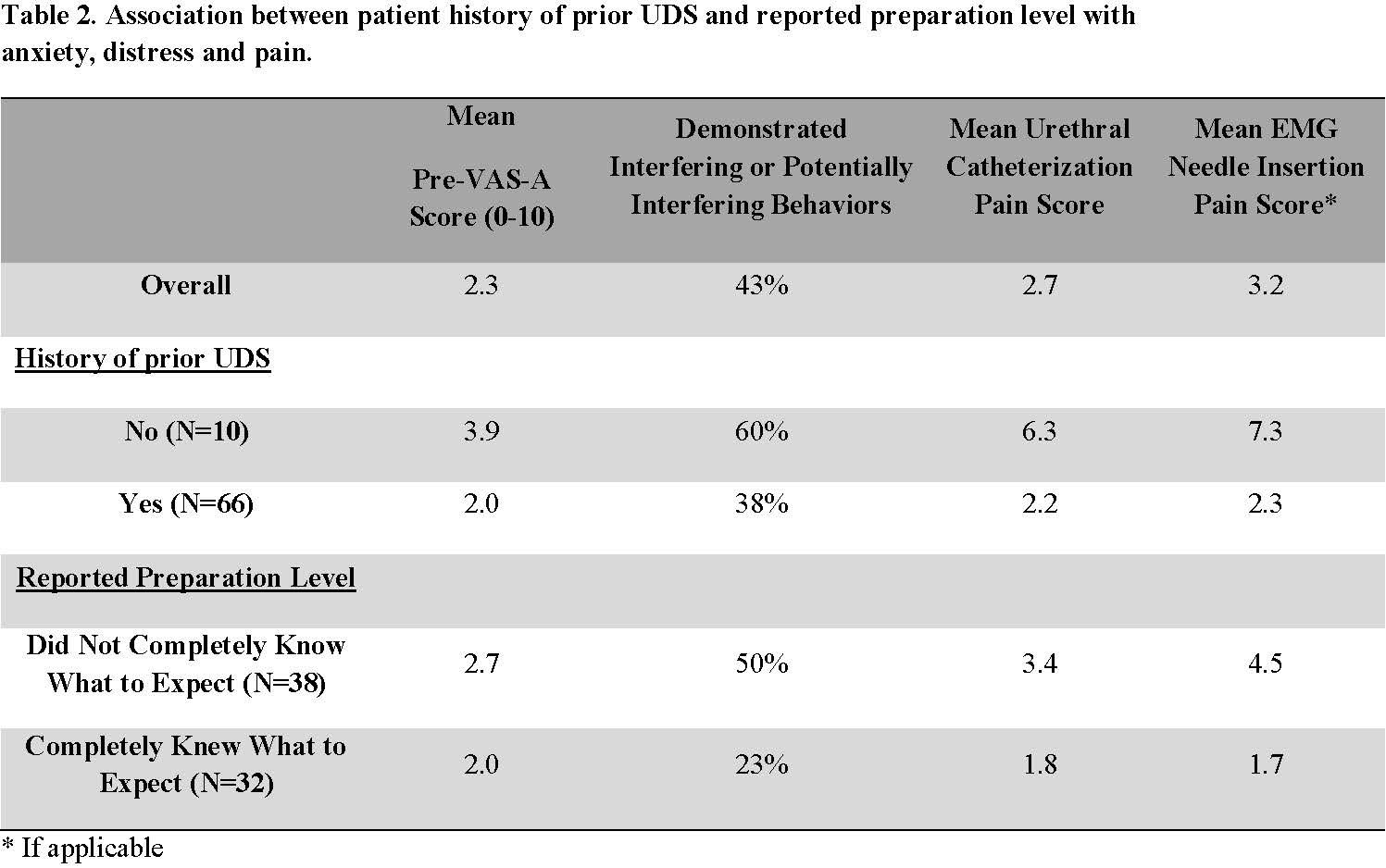
CONCLUSIONS: We found that initial testing, not knowing what to expect and undergoing EMG needle placement were associated with greater pain and distress during UDS. Our study highlights the need for resources to ease anxiety and distress for children undergoing UDS. Improved education as well as offering distraction techniques during the steps identified as eliciting the greatest pain and distress could potentially improve the pediatric UDS experience.
Back to 2019 Abstracts



