
How accurate is body surface area estimation in people with spina bifida?
Konrad M. Szymanski, MD, MPH, Chantel Colavecchia, JD, Mark P. Cain, MD, Rosalia Misseri, MD.
Riley Hospital for Children, Indianapolis, IN, USA.
BACKGROUND: Body surface area (BSA) is used to calculate renal function, doses of chemotherapy and steroids and to guide burn care. Spina bifida (SB) is associated with abnormal body habitus related to obesity, kyphosis, scoliosis and under-developed lower limbs, all of which can impact BSA. Since routine direct measurement of BSA is impractical, BSA for people with SB is calculated using formulas developed for the general population. These may be inaccurate. 3D body scanning technology has helped improve BSA equations in several studies. Our aims were 1) to evaluate differences between calculated BSA (cBSA) and measured BSA (mBSA) using 3D body scanning of children and adults with SB and 2) to determine if ambulatory status, height-arm span discrepancy and abdominal girth were associated with these differences.
METHODS: Children and adults with SB attending Multidisciplinary SB Clinics at our center were enrolled (2016-2019). cBSA was calculated using the most commonly used Mosteller formula. mBSA was obtained using the 3D Structure SensorTM, which was previously calibrated in healthy controls. Differences between cBSA and mBSA were evaluated at 5% intervals. Linear regression was used to determine predictors of BSA differences.
RESULTS: Forty-one children and 19 adults with SB (49.2% males, 41.7% community ambulators) were enrolled. Overall, 91.7% had myelomeningocele (75.0% shunted). Median mBSA was 0.005m2 (0.3%) lower than cBSA, which was not statistically significant (p>=0.12). On the other hand, only 50.0% of patients had a mBSA within 95-105% of cBSA (Table). Ambulatory status and height-arm span discrepancy were independently associated with differences between mBSA and cBSA (p<=0.04). Age, gender, girth and other anthropomorphic measurements were not associated with these differences (p>=0.12).
CONCLUSIONS: Our preliminary results indicate that compared to the BSA measured by 3D scanning, the Mosteller formula predicts BSA with greater than 5% error half of the time and with a greater than 10% error in 15% of people with SB. A SB-specific BSA formula is needed. Without it, even the most sophisticated renal function monitoring remains inaccurate. 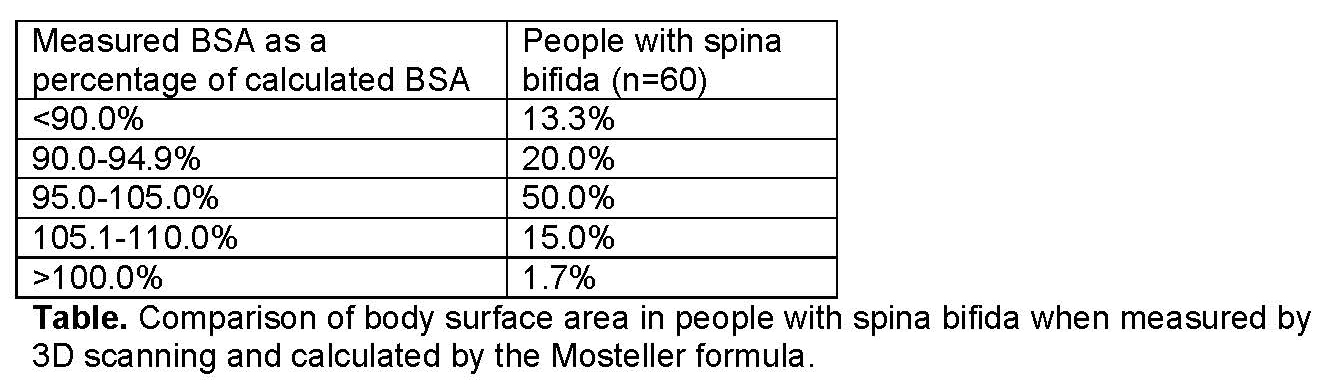
Back to 2019 Abstracts



