
Patients with disorders of sex development and the development of gonadal malignancy - risk stratification and long-term outcomes
Jacqueline Morin, MD1, Leslie Peard, MD1, Timothy Vanadurongvan, MD2, Jonathan Walker, MD2, M. Irfan Donmez, MD2, Ali M. Ziada, MD1, Amanda F. Saltzman, MD1.
1Department of Urology, University of Kentucky, Lexington, KY, USA, 2Department of Surgery, Division of Urology, University of Colorado School of Medicine, Aurora, CO, USA.
Background: Patients with disorders of sex development (DSD) have an increased risk of developing gonadal germ cell tumors (GCTs) and germ cell carcinoma in situ, gonadoblastoma (Gb). Malignancy risk in patients with DSD varies, clinical impact of Gb is poorly understood, and long-term outcomes are unknown. This study aims to review published literature to validate a malignancy risk stratification system (Looijenga et. al. 2007) and describe long-term oncologic outcomes.
Methods: A systematic PubMed review was conducted per the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement. Patients included had a DSD diagnosis and underwent gonadal biopsy or gonadectomy. Data on age at surgery, DSD diagnosis, karyotype, treatment, follow up, recurrence, and survival were analyzed. DSD diagnoses were stratified into high/intermediate, low, no, and unknown risk of gonadal malignancy based on the above mentioned stratification system. Gb/GCT and GCT-free survival by age of gonadal surgery, recurrence-free survival (RFS), and overall survival (OS) were calculated using the Kaplan-Meier method with risk groups and pathologic diagnoses compared using log-rank testing.
Results: 386 articles from 1951-2017 were included (n=2037). Median age at gonadal surgery was 17y (IQR 11-20), median follow-up was 60mos (IQR 30-68.1). Pathology revealed GCT in 11.9%, Gb in 18.1%, and no Gb/GCT in 61%.
58% of patients were high/intermediate risk. Of these, 23.8% had Gb and 21.6% GCT. In the low risk category (28%), 8.1% of patients had Gb and 10.3% had GCT. Four (<1%) patients fell in the no risk category, one had GCT. 14% of patients were of unknown risk, 20.4% with Gb and 38.5% with GCT.
Mean age with GCT at surgery was 20.7y (SD 9.8). Table shows GCT-free and Gb/GCT-free rates by age at gonadal surgery stratified by risk group.
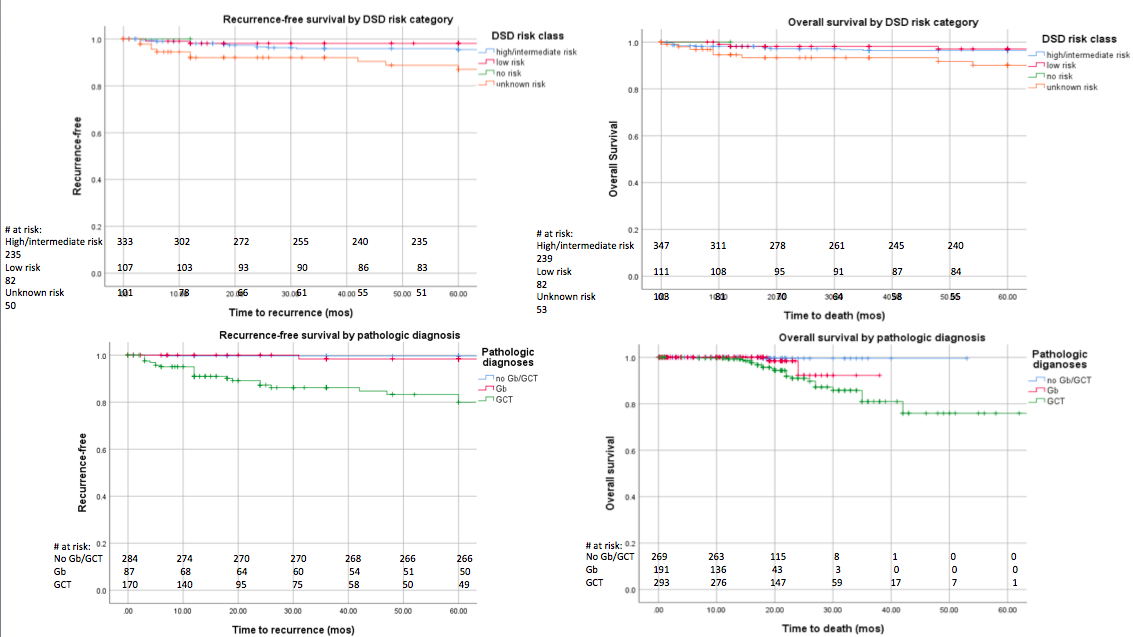
Both RFS and OS differed based on risk category and pathologic diagnosis (figure; p<0.001). Those with GCT had significantly lower 5y RFS and OS (83.3%/86.6%;
p<0.001). Those with Gb only (98.4%/96.7%) and those without abnormal pathology (99.6%/99.6%) had similar 5y RFS and OS (p>0.05).
Conclusions: While the malignancy risk classification system appears to work well, there may be DSD diagnoses excluded that carry a malignancy risk and are not adequately classified. The risk of Gb or GCT appears to increase with age, rising between 15-20y regardless of risk category. 5y RFS and OS for those with Gb is equivalent to those without Gb/GCT, regardless of risk category, but is worse for those with GCT. These data may be used when counseling families on timing of gonadal surgery and quantification of outcomes should malignancy be identified.
Table: Rate of GCT-free and Gb/GCT-free patients by age at gonadal surgery
| Risk Category | Number | % GCT-free at age at gonadal surgery | ||||||
| Patients | Events | 5y | 10y | 15y | 20y | 25y | 30y | |
| 10y | 940 | 252 | 99.6% | 97.2% | 90.6% | 68.8% | 44.5% | 33.2% |
| Low Risk | 386 | 60 | 99.7% | 99.7% | 99.1% | 91.6% | 69.4% | 67.4% |
| No Risk | 4 | 1 | 100% | 100% | 100% | 100% | 100% | 100% |
| Unknown Risk | 229 | 102 | 98.2% | 96.1% | 89.7% | 74.4% | 58.8% | 41.8% |
| Number | Gb/GCT-free at age at gonadal surgery | |||||||
| Patients | Events | 5y | 10y | 15y | 20y | 25y | 30y | |
| High/Intermediate Risk | 940 | 526 | 92.2% | 85.3% | 73.6% | 43.6% | 23.1% | 14.6% |
| Low Risk | 386 | 107 | 98.9% | 97.8% | 96.2% | 79.5% | 52.5% | 47.1% |
| No Risk | 4 | 1 | 100% | 100% | 100% | 100% | 100% | 100% |
| Unknown Risk | 229 | 150 | 92.4% | 89.5% | 82.5% | 57.2% | 40.8% | 28.6% |
Figure - 5y RFS and OS based on risk category and pathology at the time of gonadal surgery
Back to 2019 Abstracts



