
Non-animal hyaluronic acid/dextranomer gel (Deflux®) for endoscopic treatment of grade IV vesicoureteral reflux: long-term outcomes based on patient records
Anders Stenbäck, MD, PhD, Thora Olafsdottir, MD, Erik Sköldenberg, MD, PhD, Gillian Barker, MD, Göran Läckgren, MD, PhD.
Uppsala University Children's Hospital, Uppsala, Sweden.
Background: High-grade vesicoureteral reflux (VUR) is associated with a risk of febrile urinary tract infections (UTIs) and pyelonephritis. Endoscopic injection is minimally invasive and offers the chance of curing VUR while enabling avoidance of ureteral reimplantation (open surgery). Before availability of endoscopic treatment, all patients with pyelonephritis and grade IV VUR were treated by open surgery. We performed a long-term, observational study of children with grade IV VUR undergoing endoscopic injection of non-animal hyaluronic acid/dextranomer gel (Deflux®; Palette Life Sciences).
Methods: Children with grade III-V VUR and UTIs attending Uppsala University Hospital routinely received endoscopic treatment with Deflux. Criteria for endoscopic treatment were: age >1 year; persistent grade III-V VUR, diagnosed by voiding cystourethrogram (VCUG) before and after >1 year of antibiotic prophylaxis; and breakthrough febrile UTIs or poor compliance with antibiotic prophylaxis. Exclusion criteria were: endoscopic treatment with agents other than Deflux; neurogenic bladder dysfunction; previous ureteral surgery; and conditions or anomalies (other than VUR or bladder dysfunction) that affect renal or bladder function.
After endoscopic treatment, patients exhibiting grade ≥III VUR were offered repeat endoscopic treatment (maximum three procedures), or they could choose ureteral reimplantation (open surgery). In 2018 (15-25 years after endoscopic treatment), patients' charts from Uppsala University Hospital and local county hospitals were studied.
Results: Between 1 May 1993 and 30 April 2003, 185 patients (69 boys, 116 girls) were treated endoscopically and included in the current study; 237 ureters with grade IV VUR were treated. All study patients were diagnosed with VUR after pyelonephritis. The mean number of endoscopic treatments per patient was 1.46 and, in each treatment, the mean volume of Deflux injected was 0.72 mL/ureter.
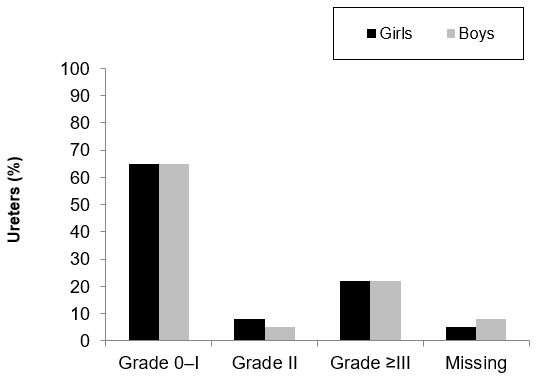
According to the last VCUG, 65% of ureters were cured (VUR grade 0-I), 7% had VUR grade II and 22% had VUR grade ≥III (Figure).
46 patients (25%; 29 females [25%] and 17 males [25%]) required ureteral reimplantation during follow-up. Of these, 41 underwent surgery 'early' (mean 6 months after the last VCUG showing persistent grade III-V VUR). Five patients underwent surgery 'late', 6-10 years after the last VCUG: one male and one female exhibited persistent VUR after treatment for lower UTI and bladder dysfunction; two females initially had obstructive refluxing megaureter (now a contraindication to endoscopic treatment); and one female developed late obstruction and had pyelonephritis 10 years after her last VCUG.
In one male, calcification around the Deflux implantation site was observed during routine examination 2 years after endoscopic treatment; no intervention was required. No further long-term adverse events or complications were apparent in any of the patients.
Conclusions: This study represents the longest ever follow-up (15-25 years) of VUR patients undergoing endoscopic treatment. Three-quarters of patients did not need ureteral reimplantation. Treatment with Deflux was durable: the risk of late clinical recurrence (UTI, persisting VUR and subsequent need for open surgery) was low.
Back to 2019 Abstracts



