
Ultrasonographic Hydronephrosis-to-Parenchyma Area Ratio in the Follow-Up of Children After Pyeloplasty
Natalia Ballesteros, M.D., Paulo R. Moscardi, M.D., Ruben Blachman-Braun, M.D., George A. Ransford, M.D., Mariarita Salvitti, M.D., Alireza Alam, M.D., Kristin A. Kozakowski, M.D., Rafael Gosalbez, M.D., Andrew S. Labbie, M.D., Miguel A. Castellan, M.D..
Nicklaus Children's Hospital, Miami, FL, USA.
Background
Success after pyeloplasty is determined by assessing the improvement of imaging studies. Ultrasounds (US) are frequently done to determine ureteropelvic junction obstruction (UPJO) improvement after intervention, with diuretic renal scans (MAG3) more commonly done in specific cases where US show similar or worsening appearance postoperatively. For this reason, we sought to evaluate the hydronephrosis-to-parenchyma area (HPA) ratio, as a more objective tool to predict success after pyeloplasty for UPJO.
Methods
We performed a retrospective chart review of all children who underwent robot-assisted pyeloplasty from 2012 to 2017. Obstruction was defined by worsening US parameters (SFU grade), abnormal curves or worsening renal function (DRF) on diuretic MAG3 renal scan, or presence of symptoms. Hydronephrosis and parenchymal areas on US before and after surgery were measured with an image processing program (imagej.nih.gov) and the HPA ratios were calculated. The HPA ratio when patients were either obstructed (preoperative and recurrences) or non-obstructed (postoperative with improvement) was used to analyze a receiver operating characteristic (ROC) curve. The most accurate HPA ratio cut-off (worrisome for obstruction vs improvement) was reported.
Results
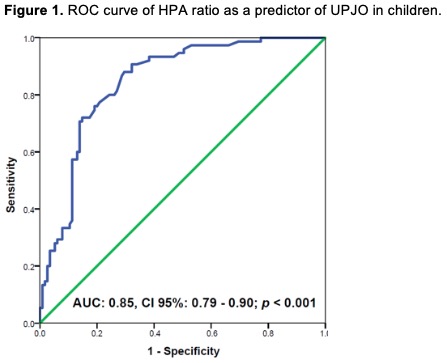
Of 110 children, 39 were excluded due to unavailable pre- or post-operative US. Table 1 depicts clinical and US variables of the 71 analyzed children. After performing a ROC curve of 190 HPA measured ratios (75 for obstruction and 115 for non-obstruction), it was shown that the higher the HPA ratio, the higher the chance that there is obstruction with an Area Under the Curve of 0.85 (p < 0.001) (Figure 1). In addition, the best cut-off HPA ratio to diagnose obstruction is 0.55 (Sensitivity: 0.72, Specificity: 0.85, Positive predictive value: 0.76, and Negative predictive value: 0.82).
Conclusions
HPA ratio is a good tool to assess hydronephrosis in children who underwent robot-assisted pyeloplasty. It can assess postoperative hydronephrosis more objectively, and aid in tailoring which patient may need additional studies such as a MAG3 scan. HPA ratio can be used to predict surgical success in children with UPJO. 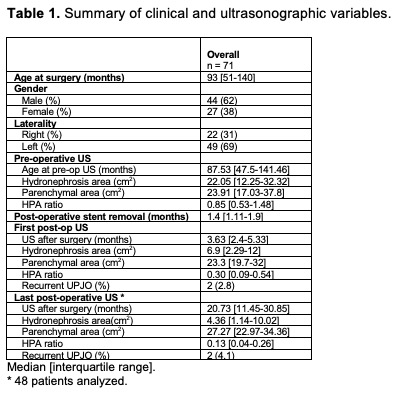
Back to 2019 Abstracts



