
Broadening candidate office circumcision patients: outcomes in children outside of conventional age and weight range
Lauren Nicassio, BS, Yuri V. Sebastiao, PhD MPH, Molly Fuchs, MD, Daryl McLeod, MD MPH, Seth Alpert, MD, Rama Jayanthi, MD, Daniel DaJusta, MD, Christina B. Ching, MD.
Nationwide Children's Hospital, Columbus, OH, USA.
Background: Office circumcision with a clamp or plastibell device is often restricted in practice by patient age and size. Recommendations often focus on children 3 months of age or less and/or weigh 5.1 kilograms (kg) or less at the time of procedure. Part of this centers on ensuring the patient fits appropriately on the restraining device and concerns of increased risk of complications. We reviewed our outcomes of office circumcision in children >3 months and >5.1 kg.
Methods: We performed a retrospective chart review of all office circumcisions performed in our urology clinic between January 2015 and August 2018 after IRB-approval. We divided the patients into two groups based on conventional age and weight cut-offs: Group 1 (≤3 months old and ≤5.1 kg) and Group 2 (>3 months old and >5.1 kg). Patient demographics and circumcision technique were recorded. Complications and need for an intervention related to circumcision were compared between groups, as well as visits to the emergency department/urgent care (ED/UC) and the office outside of those planned per follow-up protocol. Differences in outcomes were evaluated by chi-square test; a p-value <0.05 was considered significant.
Results: A total of 285 circumcisions were performed in Group 1 and 357 circumcisions were performed in Group 2. All circumcisions were performed by either gomco clamp or plastibell device. The median patient age and weight for Group 1 and 2 was 6 weeks (range 2-10) vs. 18 weeks (range 14-54) and 4.49 kg (range 2.96-5.10) vs. 6.78 kg (range 5.11-13.10 kg), respectively. Significantly more cases in Group 2 were performed with a plastibell device (77% versus 59%, p<0.0001). There was no difference in median follow-up between groups (Group 1: 17 days; range 7-140; Group 2: 16 days; range 0-181; p=0.5560). Significantly more patients in Group 2 visited the ED/UC after their procedure with a resulting intervention while there. Significantly more patients in Group 2 had a post-procedure cicatrix and required lysis of the cicatrix. There was no difference in need for operating room intervention. Plastibell malfunctions trended to be more common in Group 2 but did not reach significance. (See Table)
Conclusions: Office circumcision can be performed in patients outside of conventional age and weight ranges. The risk of post-procedure cicatrix and visits to the ED/UC in this group, however, does appear increased. These added risks, however, need to be evaluated in the context of anesthesia risk if surgical circumcision is to be offered as an alternative. Awareness of these factors are important during counseling families who desire circumcision outside of the traditional patient age and size ranges. 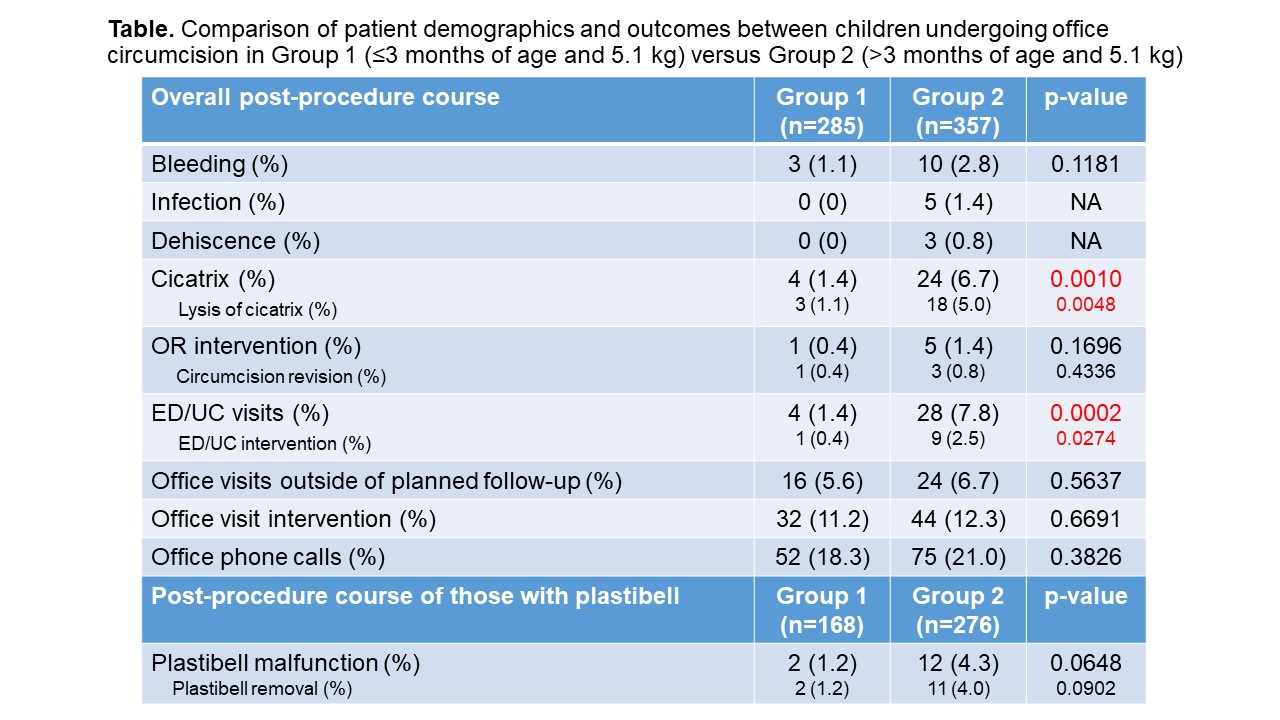
Back to 2019 Abstracts



