
Urologic Practice Patterns of Pediatricians: A Survey From a Large Tertiary Pediatric Care Center
Jonathan Gerber, MD, Alexandra N. Borden, PA-C, Angela G. Mittal, MD, Duong D. Tu, MD, Chester J. Koh, MD, Nicolette K. Janzen, MD, Ming-Hsien Wang, MD, Edmond T. Gonzales, MD, David R. Roth, MD, Paul F. Austin, MD, Abhishek Seth, MD.
Texas Children's Hospital, Houston, TX, USA.
BACKGROUND: Pediatricians are responsible for the majority of surgical subspecialty referrals. Many specialties publish guidelines with differing recommendations regarding the same pathologies. This leads to a wide variety in practice and referral patterns. The objective was to evaluate the practice patterns of pediatricians as they relate to common urologic concerns.
METHODS: A 7-question survey was created and distributed to all pediatricians at our institution. This survey dealt with pediatrician practice patterns for common urologic conditions such as urinary tract infections (UTI) and undescended testicles (UDT). Each question was multiple choice and independent of other questions in the survey. All responses were anonymous.
RESULTS: 44 of the 250 (17.6 %) providers queried responded. 89% of respondents reported performance of a comprehensive genitourinary (GU) exam at every visit while an additional 9% reported performance until adolescence. One third stated they refer UDT upon recognition at birth, 14% refer at 3 months of age, and 40% wait until 6 months of age. Testicular self-examination (TSE) was recommended at adolescence in 52%, while 33% did not recommend TSE at any age. 10% reported obtaining a voiding cystourethrogram (VCUG) after the first febrile UTI with 48% ordering one only if there were abnormal findings on renal ultrasound. 21% obtain a VCUG only after the 2nd febrile UTI is encountered and the remaining 21% prefer referral to Urology for workup. In the setting of a negative urinalysis and urine culture, 10% would provide antibiotics for UTI symptoms alone. Cefdinir was the most frequently prescribed antibiotic, followed by Bactrim. For patients who perform clean intermittent catheterization (CIC) with malodorous and cloudy urine, 38% provided antibiotics if the urine culture was also positive. 26% would only prescribe antibiotics if the patient also had systemic symptoms while 7% prescribed antibiotics for a positive urine culture in the absence of any symptoms. CONCLUSIONS: Pediatricians typically followed the AAP's guidelines regarding febrile UTIs (70%), with only a few adhering to urologic recommendations (10%). Most providers referred patients with cryptorchidism before 6 months of age or after 1 year of age, which is not consistent with either AAP or AUA guidelines. Despite a lack of supportive guidelines, most providers did recommend TSE at some point. Significant heterogeneity was noted in treating patients on CIC with suspected UTI. Despite established guidelines, practice patterns varied greatly amongst pediatricians at our institution. Harmonized, consolidated guidelines between pediatricians and pediatric urologists would improve patient care and efficiency of the healthcare system. 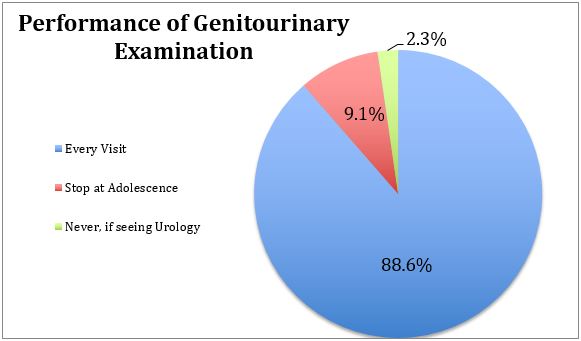


Back to 2019 Abstracts



