
Accuracy of ultrasound in identifying renal scarring as compared to DMSA scan
Julia B. Finkelstein, MD, MPH, James Rague, MD, Jeanne Chow, MD, Alyssia Venna, MBS, Meghan Shanahan, MS, Tanya Logvinenko, PhD, Caleb Nelson, MD, MPH, Richard S. Lee, MD.
Boston Children's Hospital, Boston, MA, USA.
BACKGROUND: Urinary tract infections (UTI) and vesicoureteral reflux (VUR), particularly high-grade, have been linked to the development of renal scarring (RS). 99mTc-Dimercaptosuccinic acid (DMSA) renal scan is the current gold standard for diagnosing renal scarring. We aimed to assess the accuracy of renal ultrasound (RUS) to detect renal scarring, compared to DMSA scan. Other investigators have attempted to do this but often in the setting of an acute infection or with variable, if any, exclusion of UTI.
METHODS: All initial DMSA scans performed for history of UTI or VUR in patients under 14 years old from 2006 - 2009 were identified, and clinical history obtained via chart review. We included all patients who had RUS within 4 months of the DMSA, and excluded patients with documented UTI within 4 months prior to DMSA. Findings of decreased uptake of tracer associated with loss of contours or cortical thinning defined a positive DMSA. Findings of increased echogenicity/dysplasia, cortical thinning, atrophic kidney and/or abnormal corticomedullary differentiation defined a positive RUS. The sensitivity and specificity of RUS in identifying renal scarring were calculated using DMSA scan as the gold standard.
RESULTS: 144 patients had a RUS within 4 months of the initial DMSA scan and did not have a UTI during that time period. 95/144 (66%) patients had RS on DMSA and 49/144 (34%) did not. Patients with or without RS on DMSA were not different in gender (p=0.073), age (p=0.432), insurance (p=1.000) or VUR grade (p=0.132) (Table 1). 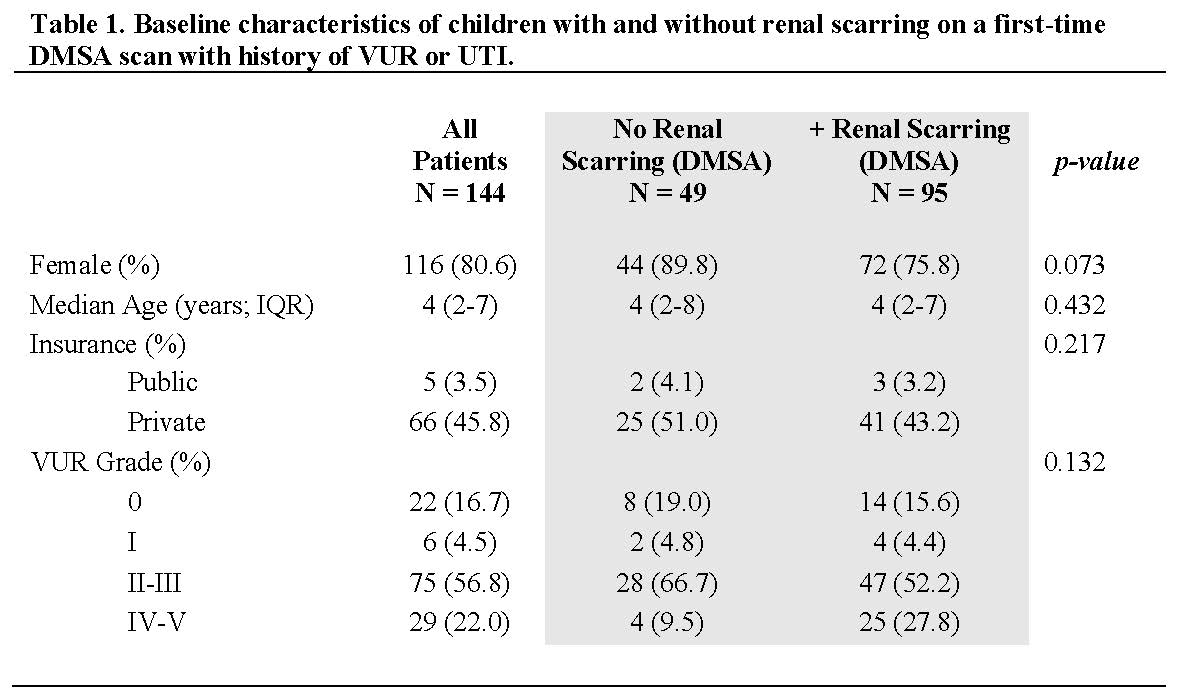
39/144 (27.1%) patients had a positive RUS, while 105/144 (72.9%) did not. The sensitivity of RUS for renal scarring was 35.8% and the specificity was 89.8%, leading to an accuracy of 54.2% (95%CI; 45.7-62.5%, p=0.999) (Table 2). 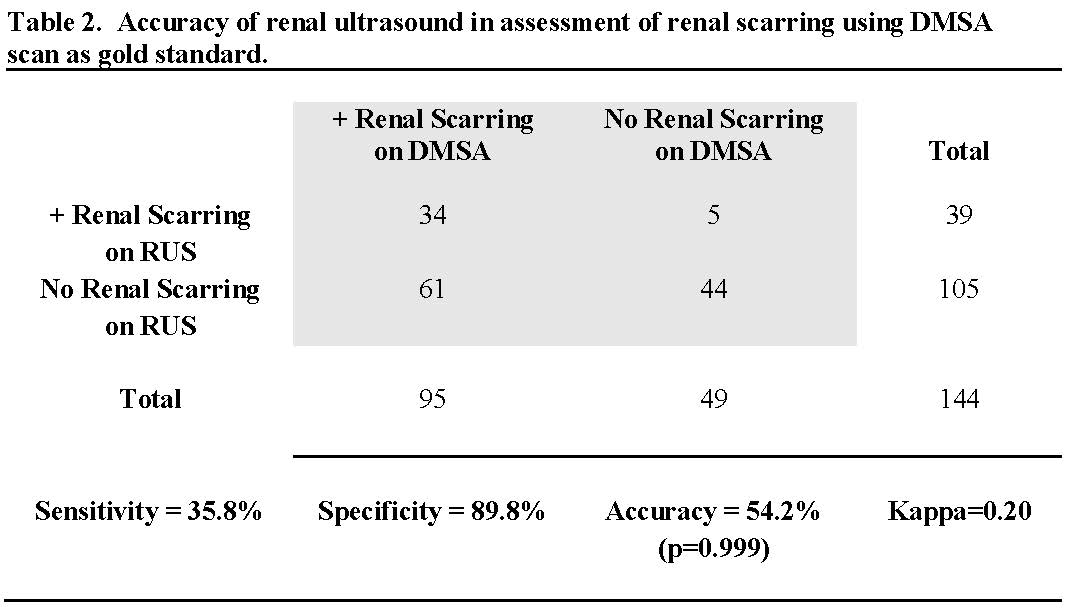
CONCLUSIONS: RUS demonstrated poor sensitivity for renal scarring visualized on subsequent DMSA. This suggests that RUS is a poor screening test for renal scarring or indicators of future renal scar. Therefore, a normal ultrasound does not necessarily rule out renal scarring or risk of future renal scar. Specificity of RUS was excellent.
Back to 2019 Abstracts



