
Delayed recognition of bladder exstrophy and persistent cloaca: an OEIS variant
Itunu O. Arojo MD1, Lynn L. Woo MD 1, 2.
1. Case Western Reserve University School of Medicine, Cleveland, OH; University Hospitals Cleveland, Medical Center, Urology Institute, Cleveland, OH; 2. Rainbow Babies and Children Hospital, Cleveland, OH.
Infant is a term female born to an otherwise healthy 31 year-old G3P2 diagnosed with an omphalocele containing the bladder on prenatal imaging (image 1A, B). On the 22 week growth scan, she was noted to have a widened pubic diastasis, possible bifid clitoris, dilated recto-sigmoid colon, and mild polyhydramnios which subsequently normalized by third trimester. At birth, an omphalocele was observed with asymmetric labia and clitoral tissue. There was an imperforate anus, and a single mucosal-lined opening in the perineum through which urine and meconium drained intermittently. Drops of urine were also seen emanating from a second, more anteriorly-located orifice within the clitoral tissue (Image2). Endoscopy confirmed the presence of a cloacal malformation with what appeared to be an intact urethra/bladder neck complex, vaginal duplication, and a fistulous tract to the rectum. A small feeding tube placed into the clitoral orifice could be seen entering the bladder separately on cystoscopy, which also appeared to show an intact bladder. Cystogram showed a smooth-walled bladder without evidence of reflux, however the infant did not void, and opacification of the urethra and common channel could not be achieved (Image 3). Spinal ultrasound was normal. On DOL 4, the omphalocele ruptured, revealing a true exstrophied bladder (Image 4). The infant remained stable and was discharged home on DOL 14, with plastic wrap covering the exposed bladder plate and diverting colostomy/mucus fistula. Cloacal repair and closure of bladder exstrophy is tentatively planned for when the infant is 6 months old.
Images:
Image 1A/B: Prenatal MRI demonstrating abdominal wall defect.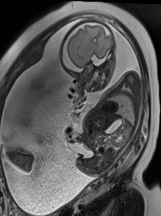
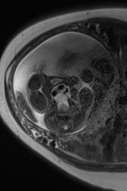
Image 2: fistulous opening in clitoris draining urine (Black arrow)
Image 3A/B: Cystogram
Image 4: Red rubber catheter through the open bladder and out through the cloaca. The feeding tube traverses the clitoral tract and exists through the exstrophied bladder.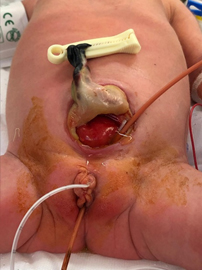
Back to 2019 SFU Program



