
Vesicoureteral Reflux Index (VURx) is Independently Predictive of Breakthrough Febrile Urinary Tract Infection in Children with Primary Reflux
Charlotte Q. Wu, MD1, Andrew J. Kirsch, MD1, Elizabeth Traore, MD1, Traci Leong, PhD2, Christopher S. Cooper, MD3, Angela M. Arlen, MD4.
1Emory University School of Medicine, Atlanta, GA, USA, 2Emory University Rollins School of Public Health, Atlanta, GA, USA, 3University of Iowa Hospitals and Clinics, Iowa City, IA, USA, 4Yale University School of Medicine, New Haven, CT, USA.
BACKGROUND: Vesicoureteral reflux Index (VURx) has been shown to reliably predict spontaneous resolution of primary reflux in children. Along with likelihood of resolution, improved identification of children at risk for recurrent febrile urinary tract infection (fUTI) may impact management decisions. We evaluated the utility of VURx as a predictive factor for breakthrough fUTI compared to VUR grade and distal ureteral diameter ratio (UDR), both of which have been reported to impact infection rates.
METHODS: Children with primary VUR and detailed voiding cystourethrogram (VCUG) were identified. A 1-6 point VURx was assigned as previously described [Figure 1]. UDR was computed by measuring largest ureteral diameter within the pelvis and dividing by the distance between L1-L3 vertebral bodies. Febrile UTI was defined as a positive urine culture of >100,000 colony-forming units (CFU) of a single organism associated with a body temperature of ≥101.5 °F. Both Random forest and logistic multivariable regression models were employed to assess the relationship (including variable importance) among VUR grade, UDR and VURx with regard to the primary outcome of breakthrough fUTI. Variable importance from the logistic regression is based on the absolute value of the t-statistic for each model parameter.
RESULTS: One hundred and thirty-nine children (94 girls, 45 boys) were analyzed with a mean age at diagnosis of 5.4 ± 4.7 years. VUR was grade 1-2 (n = 47, 33.8%), grade 3 (n = 49; 35.2%), grade 4 (30; 21.6%) and grade 5 (n = 13; 9.4%). Mean VURx was 3.24 ± 0.94; mean UDR was 0.28 ± 0.16. Mean length of follow-up was 32.1 ± 24.5 month. Thirteen children (9.4%) experienced breakthrough fUTI events. On univariate analysis, both UDR (p = 0.01) and VURx (p = 0.0005) were associated with breakthrough UTI. A random forest model was employed to ascertain which variables were considered of highest importance in predicting breakthrough fUTI, with VURx being the most important and UDR remaining significant. Logistic regression revealed the same order of importance (VURx 2.16, UDR 1.5, grade 0.16-0.76). Area under the curve (95% CI) was generated as a measure of accuracy for each variable [Figure 2], and was 0.77 (0.66-0.89) for VURx [A], 0.71 (0.56-0.86) for UDR [B] and 0.68 (0.55-0.81) for grade [B], demonstrating the superiority of VURx for predicting breakthrough fUTI.
CONCLUSIONS: Children with higher VURx are at increased risk for breakthrough febrile UTI independent of reflux grade and distal ureteral diameter ratio. VURx provides valuable prognostic information about risk of recurrent pyelonephritis facilitating individualized clinical decision-making. 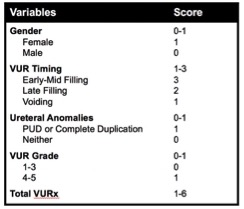

Back to 2019 Abstracts



