
Machine learning predicts individualized risk of renal complications in patients with antenatal hydronephrosis and equivocal diuretic renograms using random survival forests
David A. Ostrowski, MD1, Joseph R. Logan, MS2, Reiley Broms, BS2, Maria Antony, BS2, Mandy Rickard, NP3, Lauren Erdman, PhD, MSc3, Dennis Head, BS4, Jessica H. Hannick, MD, MSc5, Lynn L. Woo, MD5, Frederick D. Grant, MD6, Neeta D'Souza, BS2, Satish E. Viswanath, PhD7, Chris A. Flask, PhD8, Armando J. Lorenzo, MD, MSc9, Yong Fan, PhD10, Gregory E. Tasian, MD, MSc, MSCE2, John K. Weaver, MD, MSTR5.
1Division of Urology, Department of Surgery, University of Pennsylvania Health System, Philadelphia, PA, USA, 2Division of Urology, Department of Surgery, Children's Hospital of Philadelphia, Philadelphia, PA, USA, 3Division of Urology, Hospital for Sick Children, Toronto, ON, Canada, Toronto, ON, Canada, 4Northeast Ohio Medical University, Rootstown, OH, USA, Rootstown, OH, USA, 5Center for Pediatric Urology, Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA, 6Division of Radiology, Department of Surgery, Children's Hospital of Philadelphia, Philadelphia, PA, USA, 7Department of Radiology, Case Western Reserve University School of Medicine, Cleveland, OH, USA, 8Department of Radiology, Case Western Reserve University School of Medicine,, Cleveland, OH, USA, 9Division of Urology, Hospital for Sick Children, Toronto, ON, Canada, 10Department of Radiology, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA, USA.
BACKGROUND: Technetium-99m mercaptuacetyltriglycerine (MAG3) diuretic renograms are commonly utilized to evaluate suspected obstruction in patients with antenatal hydronephrosis (ANH). However, a wide range of indeterminate post-diuretic radiotracer washout half-times amongst ANH patients has been reported, making renal scan interpretation challenging. Machine learning algorithms are potential tools to improve risk assessment for these ANH patients. In this study, we sought to build machine learning models using random survival forests to analyze MAG3 renal scans and clinical variables from patients with antenatal hydronephrosis (ANH) with concern for ureteropelvic junction obstruction (UPJO) and equivocal initial MAG3 renal scans to predict risk of renal complication development. METHODS: We identified a single-center, retrospective cohort of patients under 1-year-old with ANH concerning for UPJO (Society of Fetal Urology grade ≥ 3 hydronephrosis or Urinary Tract Dilation grade ≥ 2 hydronephrosis without ureteral dilation) with an equivocal MAG3 renal scan evaluated at our institution from January 2009 until June 2021. Equivocal renal scans were studies in which the affected kidney demonstrated split function greater than 39% and the subsequent clinical recommendation was continued surveillance. Patients with history of known or suspected ipsilateral vesicoureteral reflux, bilateral UPJO, or renal anatomic abnormalities (duplicated systems, renal malrotation, renal ectopia, or horseshoe kidney) were excluded. Renal complications were defined as ≥5% decline in renal function, increased parenchymal thinning, worsening hydronephrosis, new onset flank pain, or development of pyelonephritis. Random survival forest models were constructed to predict risk of renal complications using commonly assessed clinical variables (Clinical Model), numerical features extracted from MAG3 renal scans (Imaging Model), or combining clinical and numeric renal scan features (Ensemble Model). For Clinical and Imaging models, the study sample was divided into training (80%) and testing (20%) sets, and the results were internally validated with three-fold cross-validation. The Ensemble Model was generated by averaging risk score outputs from the Clinical and Imaging models.
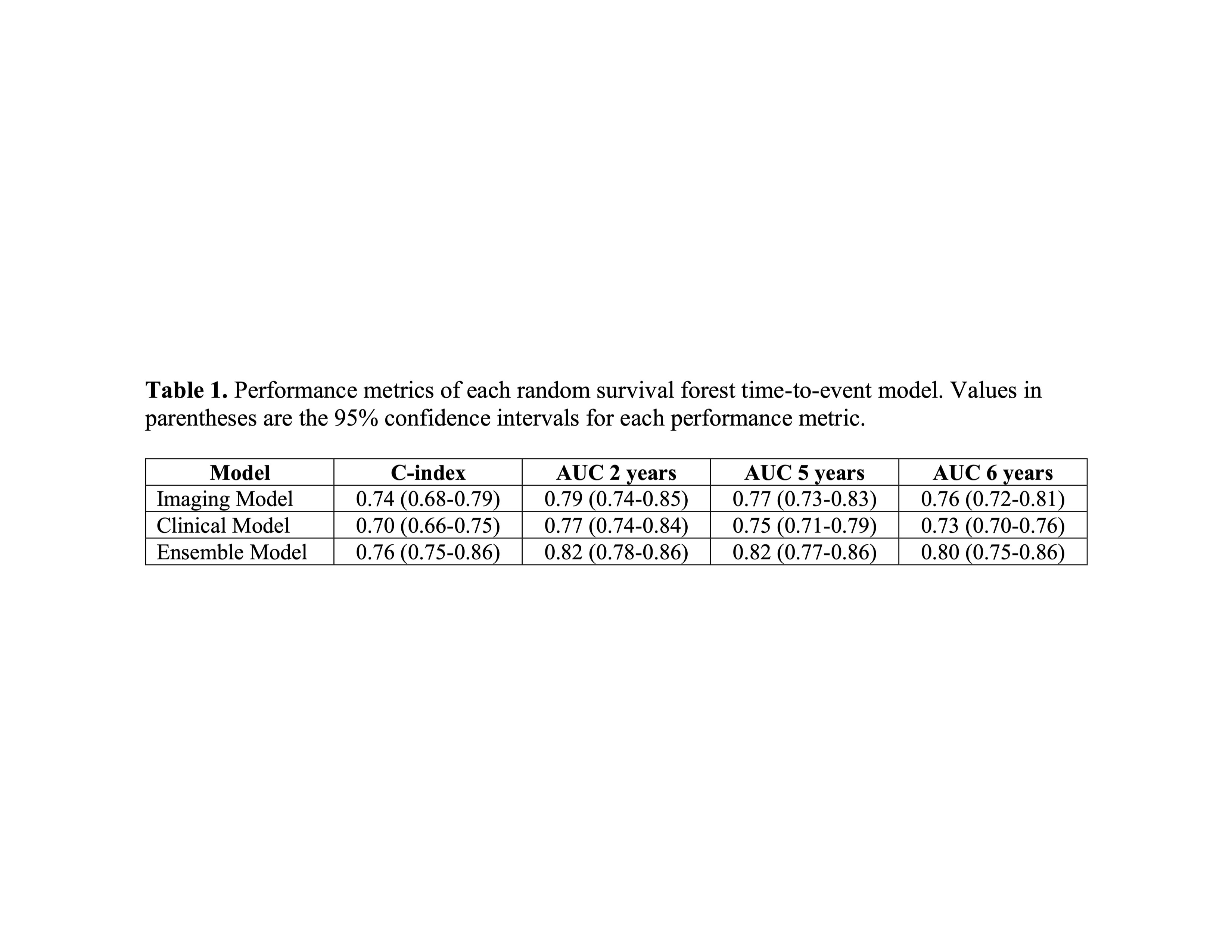
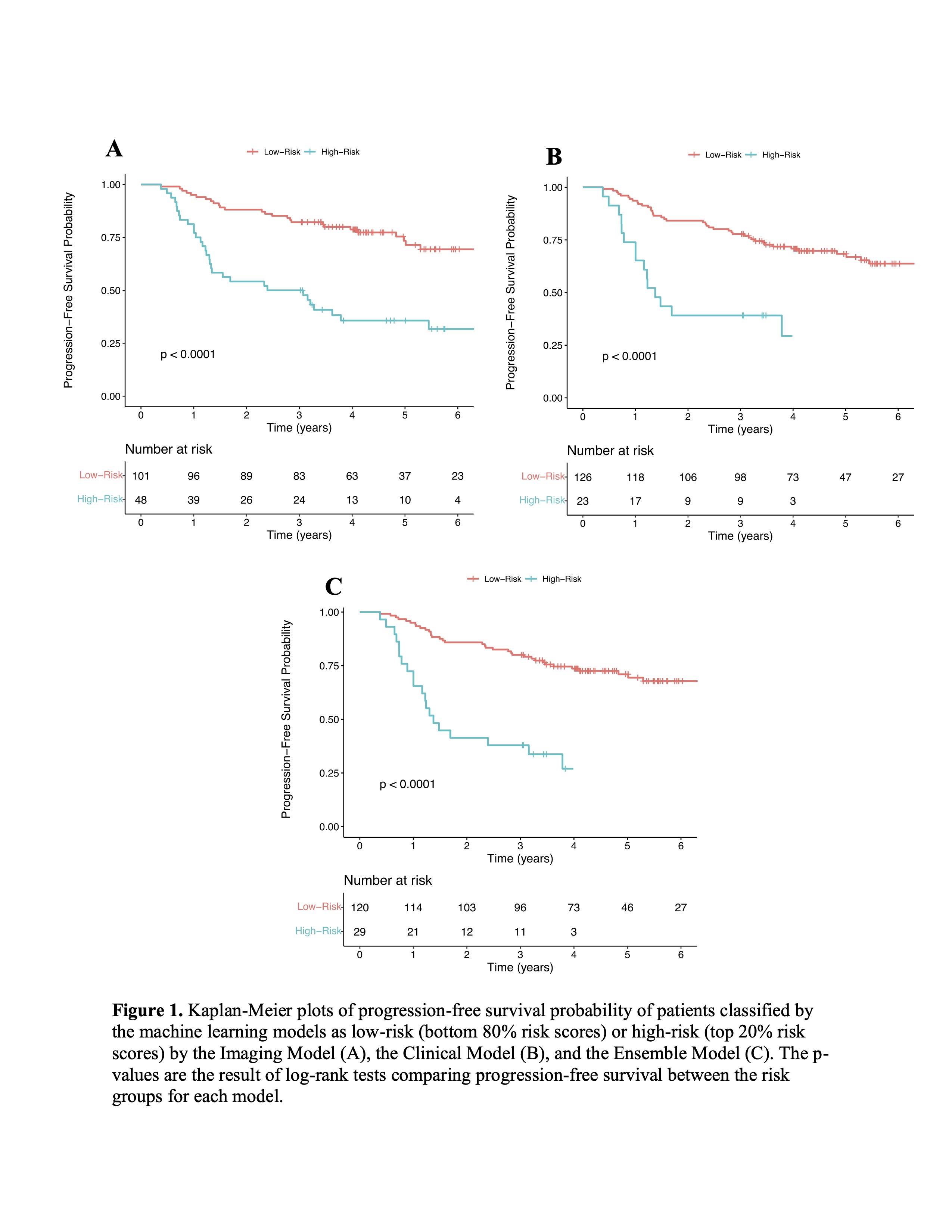
Results: One-hundred fifty-two patients were included; 62 patients developed a renal complication and 90 did not develop a renal complication with minimum 3 years follow-up. Clinical and conventional renal scan parameters were clinically similar between patients developing versus not developing a complication. The Ensemble Model (C-index 0.76; 95% CI: 0.75-0.86) demonstrated the strongest overall performance followed by the Imaging Model (C-index 0.74; 95% CI: 0.68-0.79) and the Clinical Model (C-index 0.70; 95% CI: 0.66-0.75). Differential function per unit volume of the affected kidney was the most important driver of the Clinical Model’s predictions. All models identified high-risk patients at significantly higher risk of renal complications on Kaplan-Meier log-rank analysis (p<0.0001). CONCLUSION: Random survival forest models using clinical and/or renal scan features may improve prediction of renal complication risk in patients with ANH with concern for UPJO and an equivocal initial MAG3 renal scan.
Back to 2023 Abstracts