
Pelvic Ectopic Kidney Prevalence in Cloacal Exstrophy and Pressure Changes during Second Stage Closure
Ted Lee, MD, MSc1, Elizabeth Roth, MD2, Dana Weiss, MD3, Travis Groth, MD2, John Kryger, MD2, Richard Lee, MD1, Aseem Shukla, MD3, Michael Mitchell, MD2, Joseph Borer, MD1.
1Boston Children's Hospital, Boston, MA, USA, 2Wisconsin Children's, Milwaukee, WI, USA, 3Children's Hospital of Philadelphia, Philadelphia, PA, USA.
BACKGROUND: Presence of pelvic ectopic kidney in cloacal exstrophy, also known as Omphalocele-Exstrophy-Imperforate Anus-Spinal Defects Syndrome (OEIS), has important implications during surgical reconstruction. Following a case of acute renal failure in a patient with a solitary pelvic kidney following bladder closure, our multi-institutional consortium initiated a protocol to monitor renal parameters in select children with both a pelvic ectopic kidney and an orthotopic kidney during second stage OEIS closure. We hypothesized that there would be higher elevations in renal pelvis pressure, peak systolic velocity, and resistive index in the pelvic ectopic kidney compared to the orthotopic kidney following pubic bone approximation. Furthermore, we assessed for the prevalence of pelvic ectopic kidneys within a multi-institutional OEIS cohort.
Methods: In four OEIS patients undergoing second-stage repair with known pelvic and orthotopic kidneys, renal pelvis pressure (RPP) was measured using a 4.0 French catheter connected to a fluid pressure transducer. Doppler ultrasonography was performed to measure the peak systolic velocity (PSV) of the renal artery and renal resistive index (RI) of intrarenal arteries by a dedicated pediatric radiologist. Changes in RRP, PSV, and RI in the pelvic and orthotopic kidneys following pubic bone approximation were measured. Analysis was performed using paired t-test. A multi-institutional retrospective review was performed to identify patients with OEIS and presence of pelvic ectopic kidney.
Results: Following pubic bone approximation, mean rise in renal pelvis pressure was +26.0 mmHg in the pelvic kidney and +10.3 mmHg in the orthotopic kidney (p = 0.55). One patient had immediate increase in renal pelvis pressure of 66 mmHg in the pelvic kidney but 7 mmHg in the orthotopic kidney. Once the pubic approximation stitch was relaxed, this resulted in a prompt decrease in renal pelvis pressure to 17mmHg in the pelvic ectopic kidney. Mean change in peak systolic velocity was +67.7 cm/s in the pelvic kidney compared to -25.7cm/s in the orthotopic kidney (p = 0.09). Mean change in renal resistive index was +0.06 in the pelvic kidney compared to -0.01 in the orthotopic kidney (p = 0.29). Among 80 OEIS patients, 24 (30%) had a pelvic ectopic kidney. 3 (4%) had a solitary pelvic ectopic kidney.
Conclusions: During second stage OEIS closure, we witnessed patterns of higher change in renal pelvis pressure, systolic velocity, and resistive index of the pelvic ectopic kidney compared to the orthotopic kidney. Furthermore, pelvic ectopic kidneys were found in nearly a third of OEIS patients within our multi-institutional exstrophy-epispadias complex database. Real-time renal pelvis pressure monitoring, especially those with solitary pelvic ectopic kidneys, may aid in the management of OEIS patients during the perioperative period. 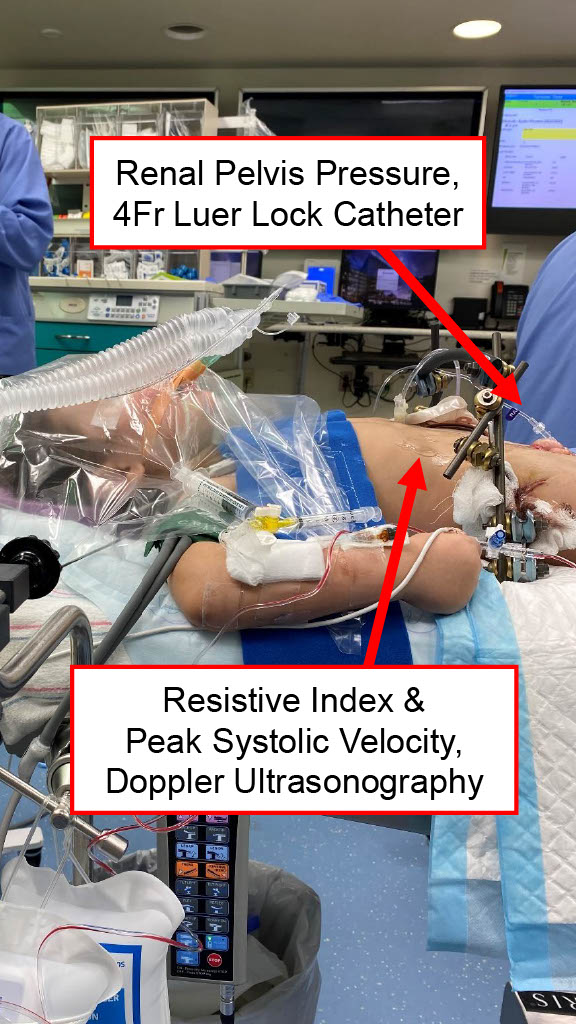
Back to 2023 Abstracts