
How effectively do we correct curvature in proximal hypospadias? - a comprehensive single institution review
Karl Godlewski, MD, Nathan Hyacinthe, BA, Katherine Fischer, MD, Sameer Mittal, MD, Jason Van Batavia, MD, Dana Weiss, MD, Arun Srinivasan, MD, Aseem Shukla, MD, Thomas Kolon, MD, Mark Zaontz, MD, Christopher Long, MD.
Children's Hospital of Philadelphia, Philadelphia, PA, USA.
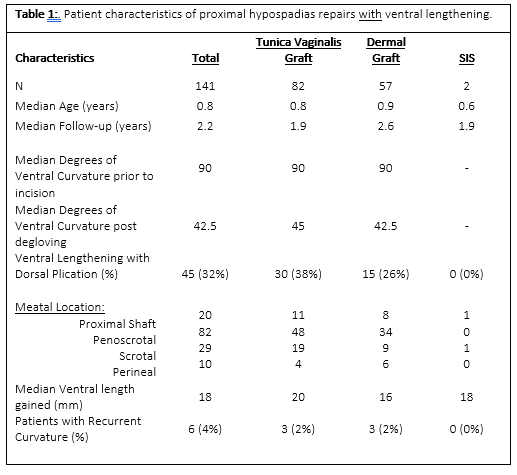
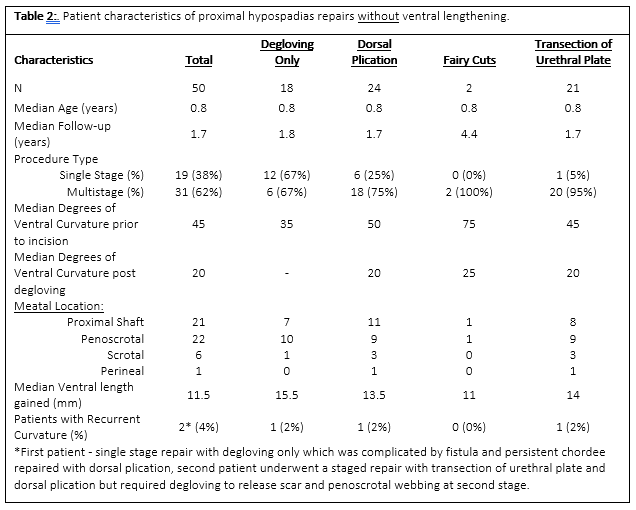
BACKGROUND: Correction of penile curvature in proximal hypospadias repair is critical to achieving a successful, durable, and functional result. Management of ventral curvature remains variable, often dictated by surgeon preference and experience. Options include penile gloving, dorsal plication, transection of urethral plate, and ventral lengthening with and without grafting. We report our comprehensive single institution experience with ventral curvature correction in patients with proximal hypospadias. We hypothesize that overall recurrence of curvature is low regardless of technique chosen, however significant differences in ventral length gained and complication exist between the various techniques. METHODS:We retrospectively reviewed our prospective surgical hypospadias registry for patients who underwent primary proximal hypospadias repair from 2016-2022. We collected information on patient age, meatal location and degree of chordee before and after degloving, preoperative and post-operative measurements of ventral penile length, procedure type, and duration of follow-up We analyzed the incidence of recurrent curvature amongst the various techniques. A descriptive analysis of outcomes was performed stratifying by type of chordee correction. RESULTS:In total, 191 patients underwent primary proximal hypospadias repair, of which 22 were single stage procedures. 141 patients required ventral lengthening with a single corporotomy and grafting including 82 TV grafts, 57 dermal grafts and 2 SIS grafts. 45 (32%) of these patients also required dorsal plication with median follow-up of 2 years (Table 1). 50 (25%) patients did not require a ventral lengthening procedure for curvature correction and had median follow-up was 1.7 years. (Table 2). Median ventral curvature prior to incision and post-degloving was 90 and 42.5 degrees in the ventral lengthening patients versus 45 and 20 degrees in the non-ventral lengthening patients, respectively. Median ventral length gained after corporoplasty with ventral lengthening procedure was 18mm compared to 11.5mm in those that did not undergo ventral lengthening. Incidence of recurrent curvature was 4% overall, 2% for TV graft, 2% DG graft , 0% SIS and 4% for no ventral lengthening. Of the 8 patients requiring repeat curvature correction, 3 were corrected with penile degloving, 3 required re-do grafting and 2 required degloving and dorsal plication. CONCLUSIONS:Overall, we found that ventral curvature is successfully corrected in 96% of patients undergoing primary proximal hypospadias repair. The use of a single ventral corporotomy with grafting in patients with corporal disproportion and severe ventral penile curvature is an effective procedure with a low rate of curvature recurrence. Median ventral length gained with this approach is 18mm. While no differences in complications were found, those that did require a ventral lengthening procedure had an overall greater gain in ventral length. Although we have a high degree of success to date, selecting appropriate techniques to correct ventral penile curvature will require continued follow up into puberty to verify outcomes.
Back to 2023 Abstracts